Whiplash Treatment in Provo, Utah
Fellowship-trained cervical trauma specialists — diagnosing the full extent of whiplash injury that standard workups miss.
What Is Whiplash?
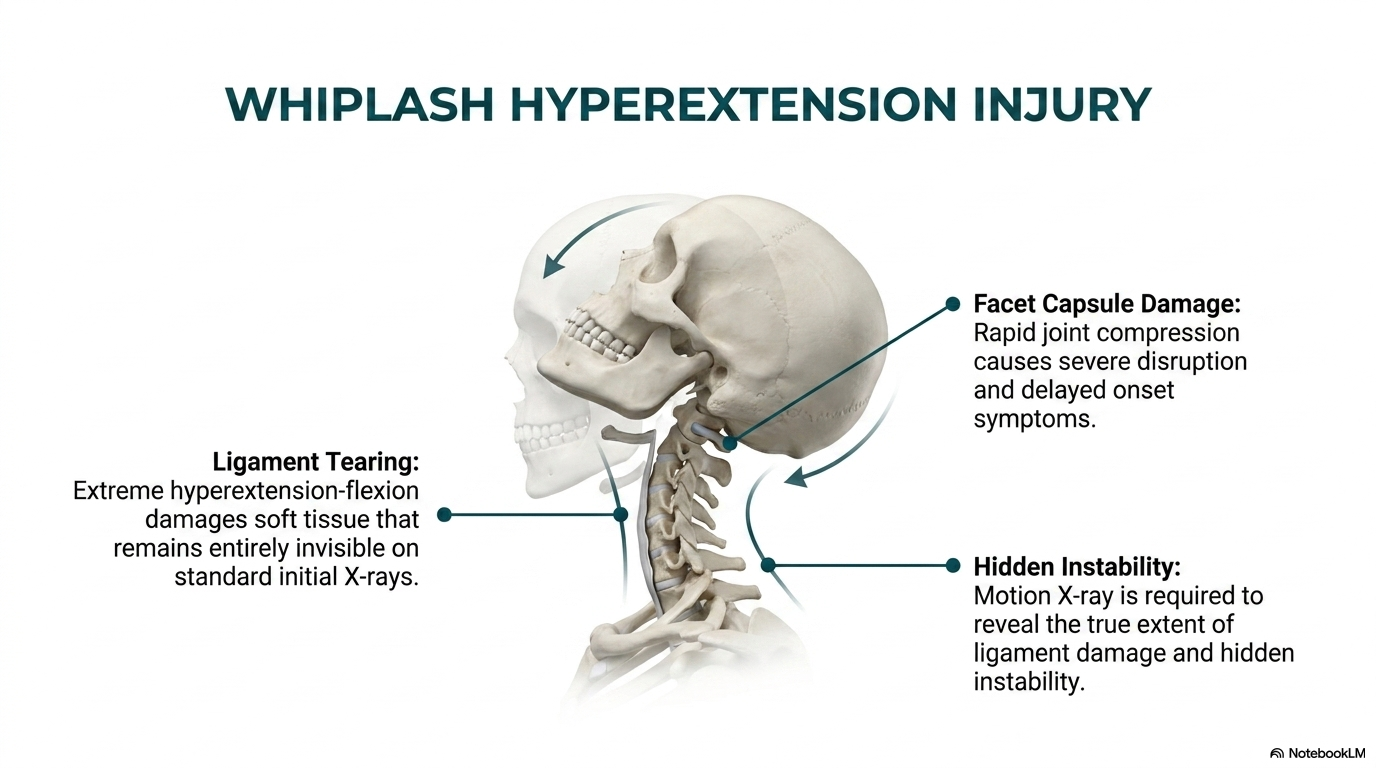
Whiplash is a cervical acceleration-deceleration injury — most commonly from rear-end collisions — where rapid, forced flexion and extension of the cervical spine produces soft tissue trauma including muscle strain, ligament sprains, disc injuries, and joint capsule damage.
The ER X-ray taken after most accidents is designed to rule out fracture — not assess ligament integrity or soft tissue injury. This means most whiplash patients are cleared from the ER with significant undiagnosed injuries still present. Ligament instability, disc herniation, and facet capsule injuries all require specialized evaluation that standard emergency workups do not include.
Untreated whiplash injuries frequently progress to chronic neck pain, headaches, arm pain, and cognitive symptoms. Early biomechanical evaluation and treatment within the first weeks after injury dramatically improves long-term outcomes.
Comprehensive Whiplash Care
Motion X-Ray for Ligament Injury
Dynamic video fluoroscopy is the only imaging modality that reveals cervical ligament instability under load. We routinely identify abnormal segmental motion at C2-C3, C3-C4, and C4-C5 that ER and standard orthopedic workups miss entirely.
MRI Interpretation
Fellowship training in MRI analysis means we review the actual imaging series for disc herniation, cord signal change, facet joint effusion, and ligament disruption — providing documentation of injury that is often critical for personal injury cases.
Cervical Rehabilitation
Treatment targets the specific injured tissues identified on evaluation: cervical adjustments for restricted segments, soft tissue therapy for muscle guarding, and postural rehabilitation to reduce chronic loading on injured ligaments.
Trauma-Trained Cervical Spine Specialists
The FSBT (Fellowship in Spinal Biomechanics and Trauma) was specifically designed to address the gap in cervical trauma evaluation and documentation. Drs. McClean’s fellowship training covers whiplash biomechanics, crash reconstruction principles, and the injury mechanisms that produce chronic cervical instability — knowledge directly applied in every whiplash case.
We work directly with personal injury attorneys throughout Utah County and have established referral relationships with local neurologists, orthopedic surgeons, and pain management specialists when escalation is indicated.
Frequently Asked Questions
My ER X-ray was normal. Does that mean I’m fine?
No. ER X-rays are taken to exclude fracture — they reveal nothing about ligament integrity, disc herniation, or soft tissue injury. Most significant whiplash injuries are invisible on standard radiographs. Patients cleared from the ER with neck pain should be evaluated by a cervical spine specialist within days, not weeks.
How soon after an accident should I be evaluated?
As soon as possible. The window for optimal recovery narrows significantly after the first 4-6 weeks. Early intervention prevents the transition from acute to chronic pain and documents the injury while findings are most acute — important for personal injury claims.
Do you work with personal injury cases?
Yes. A significant portion of our practice serves personal injury patients. We provide thorough injury documentation, work on medical liens when appropriate, and coordinate with attorneys throughout Utah County. Call 801-373-1035 for a prompt post-accident evaluation.
Clinical Evidence
Verhagen et al., 2009
A Cochrane review of conservative treatments for whiplash found moderate evidence supporting manual therapy (mobilization) and exercise over a collar alone or rest, with multimodal active interventions producing significantly better pain and function outcomes at 3 and 6 months post-injury.
Poorbaugh et al., 2008
A Pain Practice review of late whiplash syndrome identified that patients with persistent symptoms following whiplash have identifiable mechanical and neurological pathology — including ligament instability and central sensitization — that responds to directed biomechanical treatment rather than passive management strategies.
Panjabi, 1992
Panjabi’s foundational spine stability research demonstrated that ligament injury disrupts segmental stability independent of bone damage — explaining why ER X-rays miss most whiplash injuries and why dynamic assessment (motion X-ray) is essential for complete cervical trauma evaluation.
References
- Verhagen AP, et al. Conservative treatments for whiplash. Cochrane Database Syst Rev. 2009;(1):CD003338.
- Poorbaugh K, Brismée JM, Phelps V, Sizer PS Jr. Late whiplash syndrome: a clinical science overview. Pain Pract. 2008;8(2):114-129.
- Panjabi MM. The stabilizing system of the spine. Part I. Function, dysfunction, adaptation, and enhancement. J Spinal Disord. 1992;5(4):383-389.