The opioid crisis did not emerge from nowhere. It grew, in part, from a genuine problem: spine pain is common, it is often severe, and the non-pharmacological tools available to address it were not always well integrated into mainstream care. Opioids filled that gap. The consequences are well documented.
What is less discussed is what the research now shows about chiropractic access and opioid utilization. The data has become substantial enough that it warrants attention from every provider who writes prescriptions for spine pain, and from every patient who has been offered one.
What the Research Shows
Multiple large-scale studies have examined the relationship between chiropractic care access and opioid use. The findings are consistent. Patients who receive chiropractic care for spine conditions are significantly less likely to fill an opioid prescription. They are less likely to begin opioid therapy in the first place, and among those who do, the duration of use is shorter.
A 2020 study published in Pain Medicine found that among patients with spine pain diagnoses, those who saw a chiropractor had 64 percent lower odds of receiving an opioid prescription compared to those who did not. A 2018 analysis in the Journal of Alternative and Complementary Medicine found that states with higher chiropractic utilization had lower opioid prescription rates at the population level.
These are not marginal differences. They represent a meaningful population-level effect from expanding access to a non-pharmacological option.
Why the Effect Is Real
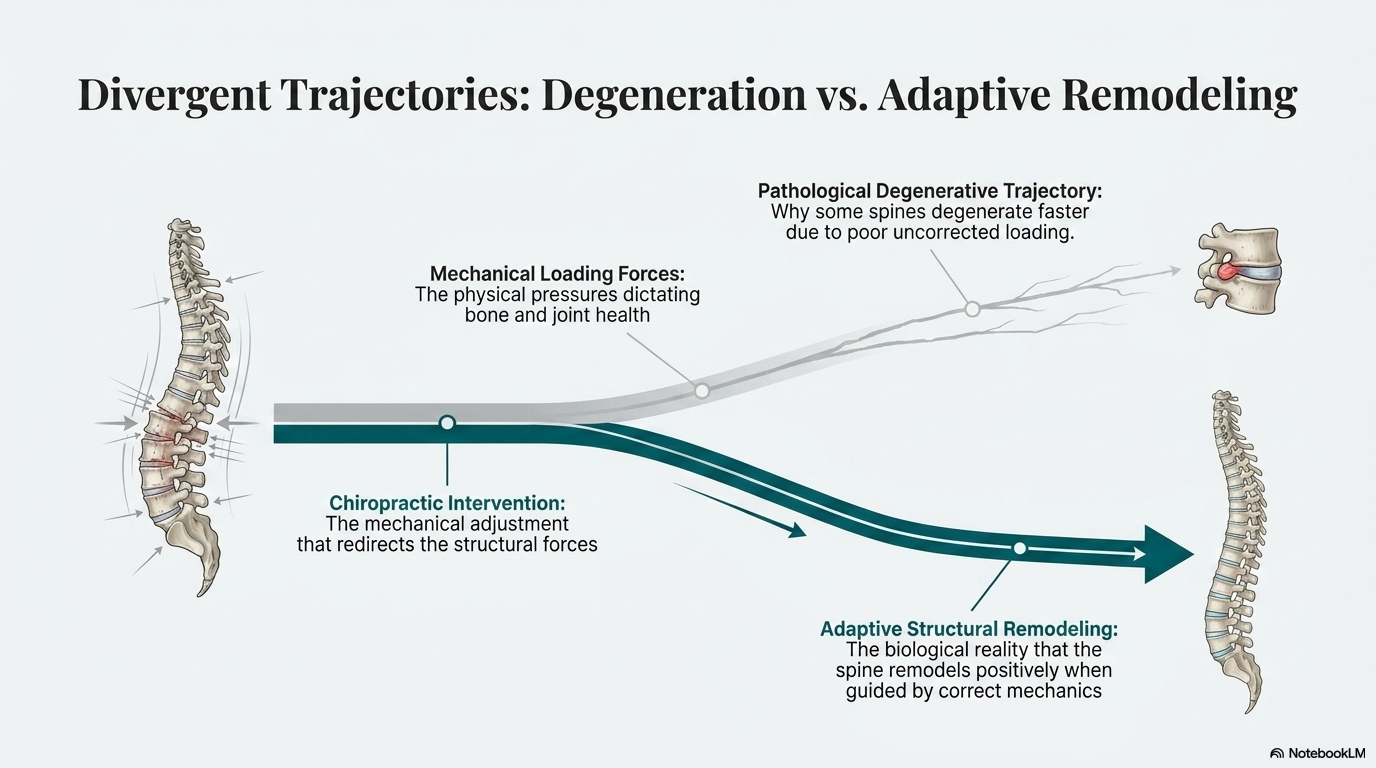
Opioids address the pain signal. They do not address the mechanical problem generating it. When a patient takes an opioid for back pain, the medication changes how the nervous system processes the pain without changing the load patterns, joint mechanics, or soft tissue tensions that are producing it. The pain may decrease. The underlying driver continues.
Chiropractic care, when it works, addresses the mechanical source. It restores joint motion, normalizes mechanoreceptor input, reduces muscle guarding, and changes the load environment that was driving the pain. When the source is addressed, the pain signal has less to report. That is a different mechanism of action than analgesic medication, and the two are not interchangeable.
For patients with mechanical spine pain, providing access to a provider who can address the mechanical cause is not a softer alternative to opioids. It is a more targeted one.
The System-level Picture
Individual prescribing decisions happen within a system. If a patient calls with acute back pain and the available options are opioids, muscle relaxants, or a referral to a provider with a several-week wait, the short-term options tend to win. This is not a failure of individual clinical judgment. It is a systems problem.
Integrating chiropractic evaluation early in the care pathway for spine pain changes those options. The patient has access to a mechanical assessment and treatment before the pain becomes chronic, before opioid dependence has a chance to develop, and before the window for effective conservative care has narrowed.
The economic argument runs in the same direction. Chiropractic care for acute spine pain costs less than the downstream costs of long-term opioid use, complex chronic pain management, and the social consequences of addiction.
For Patients Currently Managing Pain With Medication
If you are currently taking medication for spine pain and have not had a thorough biomechanical evaluation, the question worth asking is whether the mechanical source of your pain has been identified and addressed. Medication manages a signal. If the source of that signal has not been examined, managing the signal is all you are doing.
A complete evaluation, including assessment of how your spine is actually moving and loading, may identify drivers of your pain that are accessible to mechanical treatment. Resolving those changes the signal your nervous system is generating. That is a different conversation than the one about managing the signal that is already there.
What the Research Shows About Chiropractic and Opioid Use
Whedon and colleagues (2018) published a retrospective cohort study in Pain Medicine examining opioid prescribing rates among spine pain patients who initiated care with a chiropractor versus those who did not. Patients who initiated chiropractic care had a 55 percent lower probability of filling an opioid prescription within 30 days of diagnosis. The association held across age groups and pain severity levels. The study used a New Hampshire Medicaid claims database with over 18,000 patients, making it one of the larger observational studies on this question.1
Corcoran and colleagues (2020) extended this analysis in BMJ Open, using a national claims database to examine opioid initiation rates among patients with new episodes of low back pain. Patients who saw a chiropractor in the first two weeks of care had a 64 percent lower odds of receiving an opioid prescription compared to those who did not receive chiropractic care. The effect was largest for patients under 45 years of age, the demographic at highest risk for transitioning from prescription opioid use to dependence.2
The mechanism behind these findings is straightforward. If a mechanical spine problem responds to manipulation, the patient does not need pain medication at the same level. More importantly, early resolution of the mechanical driver reduces the likelihood of central sensitization and chronic pain development, which is the pathway that leads to long-term opioid dependence. A 2019 systematic review in JAMA Network Open by Skelly and colleagues found moderate-to-high strength evidence for non-pharmacological approaches including spinal manipulation for acute and chronic low back pain, reinforcing the argument that these approaches should be offered earlier in the treatment pathway, not as a last resort after pharmacological management has failed.3
References
- Whedon JM, Toler AWJ, Goehl JM, Kazal LA. Association between utilization of chiropractic services for treatment of low back pain and opioid receipt. Pain Med. 2018;19(9):1774-1781.
- Corcoran KL, Bastian LA, Gunderson CG, Steffens C, Brackett A, Lisi AJ. Association between chiropractic use and opioid receipt among patients with spinal pain. J Altern Complement Med. 2020;26(6):490-494.
- Skelly AC, Chou R, Dettori JR, et al. Noninvasive nonpharmacological treatment for chronic pain: a systematic review. JAMA Netw Open. 2020;3(7):e2014484.
- Martin BI, Deyo RA, Mirza SK, et al. Expenditures and health status among adults with back and neck problems. JAMA. 2008;299(6):656-664.
Ready for a Complete Biomechanical Evaluation?
Schedule with Dr. McClean at McClean Chiropractic in Provo, Utah. Fellowship-trained. Biomechanics-focused. The most advanced spine assessment in Utah County.