There is a window in the early weeks of a spine problem when the outcome can still go either direction. That window does not stay open indefinitely. What happens in that period often determines whether pain resolves or becomes something a patient will manage for the rest of their life.
Most people do not know that window exists. Most care systems do not treat it as the priority it is.
From Acute to Chronic: What Changes
Acute pain and chronic pain are not the same condition at different stages. They are physiologically distinct. Acute pain is a signal, the nervous system reporting tissue stress or damage. Chronic pain involves changes in how the nervous system itself processes that signal. The threshold drops, the response amplifies, and eventually the system generates pain that is no longer proportional to what is happening in the tissue.
This process is called central sensitization, and it follows a predictable course. Repeated nerve signals cause the spinal cord’s pain-processing neurons to fire more easily over time. The brain reorganizes how it maps and interprets the painful area. The brain’s own system for dampening pain signals becomes less effective. What begins as a mechanical problem in the spine can evolve into a neurological one that is significantly harder to treat.
The critical point is that this transition happens in a window. It is not inevitable.
Why Mechanical Problems Drive the Transition
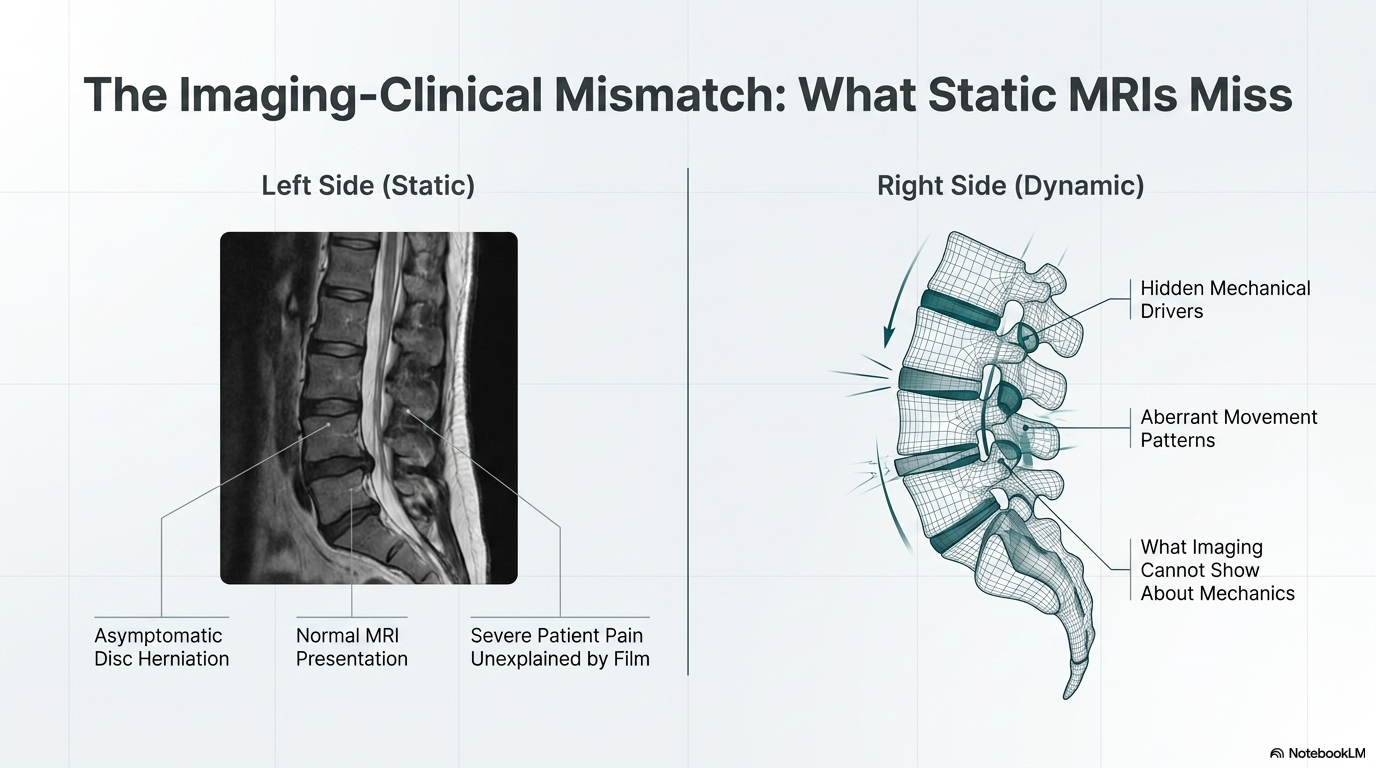
When a spinal segment is not moving correctly, it creates a persistent source of abnormal input into the nervous system. The mechanoreceptors in the joint capsules and surrounding tissues send continuous signals upward. If that input is not resolved, it contributes to the sensitization process over time.
The patients most at risk are the ones who manage symptoms in the early phase without addressing the underlying mechanical problem. They take something for the pain, the acute phase settles down, and they return to normal activity. But the mechanical driver that created the original problem is still there, still generating abnormal input, still loading the spine in a pattern that has not changed. The nervous system keeps receiving that signal. At some point the system stops recovering the way it did the first time.
What Early Intervention Actually Does
Restoring normal segmental motion in the early phase of a spine problem does more than relieve pain. It changes the input the nervous system is receiving. Joints that move correctly generate appropriate mechanoreceptor signals. The abnormal stream that was feeding the sensitization process gets interrupted. The tissue stress driving inflammation decreases.
This is why timing matters. The same intervention that works effectively in the first few weeks becomes progressively less efficient once central sensitization is established. It is not that it stops working. It is that the problem has grown a layer more complex, and that layer requires more time and more work to address.
What This Means If You Are in Pain Right Now
Waiting to see if pain resolves on its own is reasonable for minor and brief episodes. But when spine pain does not begin to improve within a few weeks, or when it keeps coming back, that is a signal that something mechanical is driving it and that the window for straightforward intervention is still open.
The evaluation process matters here. A thorough biomechanical assessment identifies the mechanical driver, not just the location of the pain. Where something hurts and what is causing it are not always the same place in the spine. Treating the right area at the right time is what separates outcomes that hold from outcomes that do not.
Chronic spine pain is not just acute pain that lasted longer. It is a different problem, and preventing it requires acting during the phase when the spine still responds efficiently to mechanical correction. That phase is real, it is identifiable, and it has an end.
The Research on the Acute-to-Chronic Transition
The transition from acute to chronic pain is not simply a matter of time passing. It involves measurable neurological changes in the spinal cord and brain. Woolf (1983) described wind-up, the progressive amplification of spinal cord neuron responses to repeated nociceptive input, as a mechanism by which acute pain states become self-sustaining. With sufficient repetitive nociceptive input, the threshold for pain signaling in the dorsal horn drops permanently, and stimuli that would not normally produce pain begin to do so. This central sensitization is not hypothetical. It is detectable on functional MRI and measurable by quantitative sensory testing.1
Moseley and colleagues have published extensive work on the role of central sensitization in low back pain. A 2003 paper in Pain demonstrated that patients with chronic low back pain show altered cortical representation of the back in the somatosensory cortex, a finding that does not reverse with rest or medication alone, but that does respond to treatments that involve both sensory input and motor re-education.2 This research suggests that the window for preventing central sensitization from becoming established is real, and that what happens in the first four to eight weeks of an acute spine problem shapes the neurological environment for long-term recovery.
Linton (2000) published a systematic review in Spine of 37 prospective studies examining risk factors for chronic disability following acute back pain. The strongest predictors of chronicity were not severity of initial injury but psychological and behavioral factors: fear-avoidance beliefs, catastrophizing, job dissatisfaction, and prior episodes of back pain. Importantly, early intervention that addresses movement behavior and pain beliefs, which is what a properly conducted course of chiropractic care does, is associated with significantly lower rates of chronicity at one-year follow-up.3
References
- Woolf CJ. Evidence for a central component of post-injury pain hypersensitivity. Nature. 1983;306(5944):686-688.
- Moseley GL, Zalucki N, Birklein F, Marinus J, van Hilten JJ, Luomajoki H. Thinking about movement hurts: the effect of motor imagery on pain and swelling in people with chronic arm pain. Arthritis Rheum. 2008;59(5):623-631.
- Linton SJ. A review of psychological risk factors in back and neck pain. Spine. 2000;25(9):1148-1156.
- Vlaeyen JWS, Linton SJ. Fear-avoidance and its consequences in chronic musculoskeletal pain: a state of the art. Pain. 2000;85(3):317-332.
Ready for a Complete Biomechanical Evaluation?
Schedule with Dr. McClean at McClean Chiropractic in Provo, Utah. Fellowship-trained. Biomechanics-focused. The most advanced spine assessment in Utah County.