Most people describe back pain in vague terms. Something is out. Something is tight. Something does not feel right. Those descriptions are more accurate than they realize. What they are pointing to, without knowing the clinical language for it, is segmental dysfunction. And understanding what that actually means changes how you think about your spine and your care.
What a Spinal Segment Is
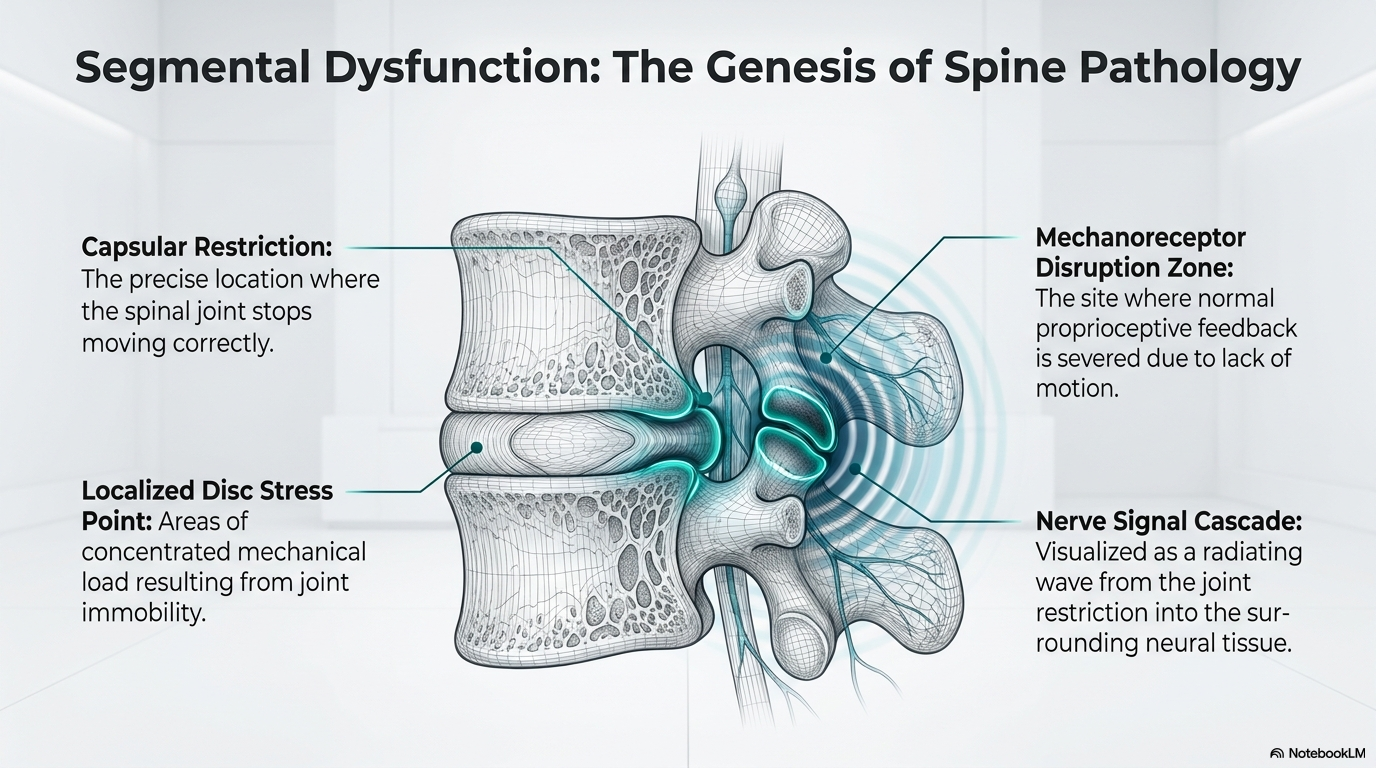
Your spine is made up of individual motion segments, each one consisting of two vertebrae, the disc between them, and the two small joints at the back called facet joints. Each segment is designed to move through a specific range in multiple directions. When that movement is working correctly, the segment does its job quietly. You do not notice it.
When movement at a segment is lost, excessive, or abnormal, the whole picture changes. That is segmental dysfunction, and it sets off a cascade that explains most of what patients experience as back pain.
The Cascade That Follows
Inside the facet joint capsule and the surrounding soft tissue are mechanoreceptors, nerve endings that are constantly reporting information upward to the spinal cord and brain. Their job is to tell the nervous system exactly where the joint is, how it is moving, and what forces are passing through it. That information is used at every level of the nervous system to coordinate posture, movement, and muscle activation.
When a joint is not moving correctly, the quality of that information changes. The nervous system receives an abnormal signal. It responds by increasing muscle tension around the affected segment, which is an attempt to protect it. That increased tension further restricts movement. The disc between the vertebrae, which depends on movement to stay hydrated and healthy, begins to receive less fluid exchange. Pressure patterns in the joint change. The altered movement affects how forces transfer through adjacent segments, which now have to compensate for what the dysfunctional one is not doing.
This is not a dramatic injury. It is a quiet functional failure that compounds over time.
Why It Does Not Show On an MRI
Segmental dysfunction is a movement problem, not a structural one. An MRI captures structure. It shows the bones, the discs, the nerves. It does not show whether a joint is moving correctly or what signals it is sending into the nervous system. A segment can be profoundly dysfunctional without producing a single finding on imaging.
This is one reason why some patients have significant pain with a relatively unremarkable MRI. The problem is real. The test simply is not designed to find it.
What Restoring Motion Actually Does
When normal segmental motion is restored, the mechanoreceptor signal normalizes. The nervous system receives accurate information. The protective muscle guarding decreases. The disc begins to cycle fluid normally again. The forces that were being abnormally transferred to adjacent segments reduce.
The effect is not just mechanical. Restoring joint motion generates a specific type of nerve input that inhibits pain signals at the spinal cord level. This is part of why manual treatment to a specific segment often produces immediate pain relief that extends beyond that segment. The nervous system’s response to restored motion is broader than the joint itself.
What This Means for How You Are Treated
Identifying which segments are dysfunctional, and in what way, is the foundation of a biomechanical evaluation. Not every painful area in the spine is the source of the dysfunction driving it. The spine is a connected system, and forces transfer predictably from one region to another. A segment that is not moving correctly in the mid-back will change how the lower back is loaded. A problem in the lower back will affect how the pelvis and hips function.
Effective care starts with finding the actual source of the dysfunction, not just the area that hurts. That requires hands-on assessment and, when indicated, motion X-ray to evaluate how specific segments are moving under load. From there, treatment can be aimed at the right target.
What The Research Says About Segmental Dysfunction
The concept of a neutral zone offers a precise framework for understanding what changes when a spinal segment loses normal function. Panjabi defined the neutral zone as the region of intervertebral motion around the neutral posture where minimal internal resistance is encountered. When this zone increases in size, it is a sign of mechanical instability; when it is pathologically restricted, the mechanoreceptive signaling from that segment is altered. His two-part paper in the Journal of Spinal Disorders (1992) remains one of the most cited works in spinal biomechanics and provides the theoretical basis for why a single restricted or hypermobile segment can drive global dysfunction throughout the spine.1,2
The facet joint capsule is the most mechanoreceptor-dense structure in the posterior spine. Wyke’s foundational research demonstrated four distinct types of mechanoreceptor endings in the facet capsules and spinal ligaments, each responsible for different aspects of proprioceptive and nociceptive signaling. Type I endings provide continuous postural information. Type II endings respond to movement onset. Type III endings signal end-range position. Type IV are pain receptors that activate when tissue is mechanically stressed or chemically irritated.3 When a segment is restricted, Type I and II signaling is disrupted, and over time Type IV receptors become sensitized. This is the neurological mechanism behind chronic joint-level pain that does not respond to rest or medication.
Solomonow and colleagues (2003) described the consequence of ligament subfailure injury (injury below the threshold of frank tearing) on the muscular stabilization system. When spinal ligaments are overstretched or repetitively loaded beyond their elastic range, the reflex arc between the ligament’s mechanoreceptors and the surrounding musculature is disrupted. The muscles guarding that segment lose their coordinated response pattern. This research explains why a segment that has been mechanically stressed, even without visible structural damage on imaging, can produce persistent dysfunction that exercise alone cannot resolve.4
References
- Panjabi MM. The stabilizing system of the spine. Part I. Function, dysfunction, adaptation, and enhancement. J Spinal Disord. 1992;5(4):383-389.
- Panjabi MM. The stabilizing system of the spine. Part II. Neutral zone and instability hypothesis. J Spinal Disord. 1992;5(4):390-397.
- Wyke B. Articular neurology and manipulative therapy. In: Glasgow EF, et al., eds. Aspects of Manipulative Therapy. 2nd ed. Churchill Livingstone; 1985:72-77.
- Solomonow M, et al. A hypothesis of chronic back pain: ligament subfailure injuries lead to muscle control dysfunction. Eur Spine J. 2003;12(5):457-479.
Ready for a Complete Biomechanical Evaluation?
Schedule with Dr. McClean at McClean Chiropractic in Provo, Utah. Fellowship-trained. Biomechanics-focused. The most advanced spine assessment in Utah County.