Two people, same age, same general health, similar activity levels. One of them has a spine that moves well and causes minimal problems into their 60s and 70s. The other has been managing chronic back pain for years and is facing significant degenerative changes at multiple levels. The difference between them is real and it has an explanation. It is not mostly luck, and it is not mostly genetics.
It is largely mechanical.
What Degeneration Actually Is
Spinal degeneration is the process by which the structural components of the spine break down over time. Discs lose height and hydration. Facet joints develop arthritic changes. Ligaments thicken. Bone spurs form. These changes are real and they show clearly on imaging.
What imaging does not show is why they happened at that rate, at those levels, in that patient.
Degenerative changes are not distributed randomly through the spine. They concentrate at specific levels, and the pattern of concentration follows the pattern of abnormal mechanical stress. The segments that are loaded asymmetrically, that are restricted in their motion, or that are bearing compensatory forces from dysfunction elsewhere in the spine are the ones that break down first and fastest.
The degeneration is not the cause of the problem. It is the record of where abnormal mechanical forces have been concentrated over years or decades.
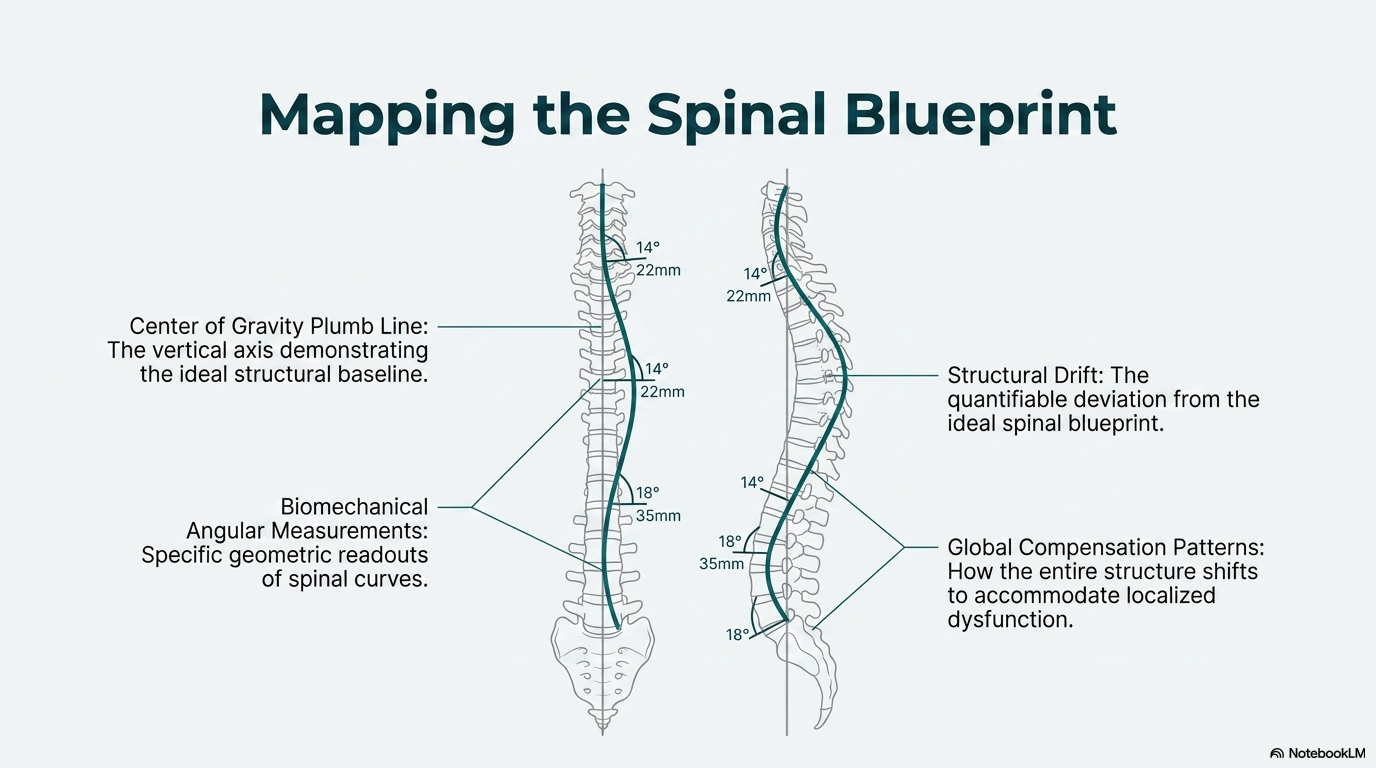
The Blueprint and the Drift
Every spine has a structural blueprint, fixed bony angles in the pelvis and the base of the neck that define what the spinal curves should look like for that individual. When the spine maintains its alignment near that blueprint, forces distribute reasonably evenly across the discs and joints. The load is shared. No single level bears a disproportionate burden.
When posture drifts from the blueprint, whether from injury, from years of occupational loading, or from accumulated habits, the force distribution changes. The pelvis tilts backward. The mid-back rounds. The head shifts forward relative to the hips. Each shift concentrates load at specific levels and in specific tissues. The structures bearing that concentrated load begin to show the consequences over time.
The drift does not happen overnight. Neither does the degeneration. But the process is continuous, and the cumulative effect over decades is significant. The patient who ends up with severe multilevel degeneration in their 50s did not develop it suddenly. It was building through the mechanical environment their spine was living in for years before the imaging showed it.
The Window for Intervention
Degeneration that has already occurred cannot be reversed. Bone spurs do not resolve. Lost disc height does not return. But the rate of further degeneration is not fixed, and the trajectory of a spine that is currently heading toward accelerated breakdown is modifiable.
The intervention that changes that trajectory is mechanical. Restoring normal segmental motion at restricted levels changes the load distribution. Correcting postural drift toward the structural blueprint reduces the concentration of forces at the levels bearing disproportionate stress. Maintaining that correction over time changes the mechanical environment the spine is living in.
The discs and joints of a spine that moves correctly and loads symmetrically age differently than those of a spine that does not. The structural components are the same. The mechanical environment they are subjected to determines how quickly and how severely they change.
What This Means for People Without Symptoms Yet
The most important time to evaluate and address spinal mechanics is before significant symptoms develop, not after. A spine that is drifting from its blueprint and beginning to show early degenerative changes at specific levels is at a fork in the road. The path it takes from that point depends on whether the mechanical factors driving the drift are identified and addressed.
Most people do not come in for evaluation until the pain becomes significant. By that point, the degeneration that is visible on imaging has been accumulating for years. The care at that stage is still valuable and still changes the trajectory. But the opportunity that existed earlier, to address the mechanical environment before significant structural change occurred, is gone.
Understanding your spine’s mechanics, where it sits relative to its blueprint, how it is loading, which segments are functioning correctly and which are not, is the basis for a proactive relationship with your spine rather than a reactive one. The patients who manage their spine well over a lifetime are almost always the ones who developed that understanding early and acted on it.
The Mechanical Basis of Differential Disc Aging
The intervertebral disc has no direct blood supply after early childhood. Its nutrition depends entirely on diffusion through the cartilage endplates, a process that is highly sensitive to compressive loading patterns. Nachemson’s work on intradiscal pressure established that the disc experiences dramatically different compressive loads depending on body position and activity: pressure in the disc increases by more than 200 percent from lying supine to sitting unsupported. Asymmetric or repetitive loading, particularly the kind generated by abnormal spinal mechanics, concentrates this compressive force on specific regions of the disc, accelerating the breakdown of the nucleus and annulus in those regions while leaving adjacent areas relatively intact.1
Roughley (2004) published a thorough review of the biochemical mechanisms of disc degeneration in Spine, summarizing the evidence that mechanical loading patterns directly influence the expression of degradative enzymes (matrix metalloproteinases) in disc tissue. Normal cyclic loading within physiological ranges maintains disc cell viability. Abnormal loading patterns, whether from chronic compression, torsional stress, or reduced motion, shift the cellular environment toward a catabolic state in which the structural proteins of the disc are broken down faster than they can be replaced.2
Twin studies have provided the most direct evidence for the relative contributions of genetics versus mechanics in disc degeneration. Battie and colleagues (2008) examined lumbar disc degeneration in 1,474 male twin pairs using MRI grading. While genetic factors accounted for approximately 61 percent of disc degeneration variance in the lower lumbar spine, occupational loading, lifetime physical exposures, and body weight explained meaningful additional variance. And crucially, these are all modifiable factors.3 The genetic predisposition determines your starting point. The mechanical environment you create through posture, alignment, and activity determines whether your disc ages at the rate of the best-case or worst-case scenario within that predisposition.
References
- Nachemson A. Disc pressure measurements. Spine. 1981;6(1):93-97.
- Roughley PJ. Biology of intervertebral disc aging and degeneration: involvement of the extracellular matrix. Spine. 2004;29(23):2691-2699.
- Battie MC, Videman T, Kaprio J, et al. The Twin Spine Study: contributions to a changing view of disc degeneration. Spine J. 2009;9(1):47-59.
- Urban JPG, Roberts S. Degeneration of the intervertebral disc. Arthritis Res Ther. 2003;5(3):120-130.
Ready for a Complete Biomechanical Evaluation?
Schedule with Dr. McClean at McClean Chiropractic in Provo, Utah. Fellowship-trained. Biomechanics-focused. The most advanced spine assessment in Utah County.