Headache Treatment in Provo, Utah
Identifying the cervical and biomechanical causes of headaches — not just treating the pain.
Yes, chiropractic care helps many headaches, especially those that start in the neck. Our Provo doctors find the source and treat it rather than masking the pain.
Cervicogenic and Tension Headaches
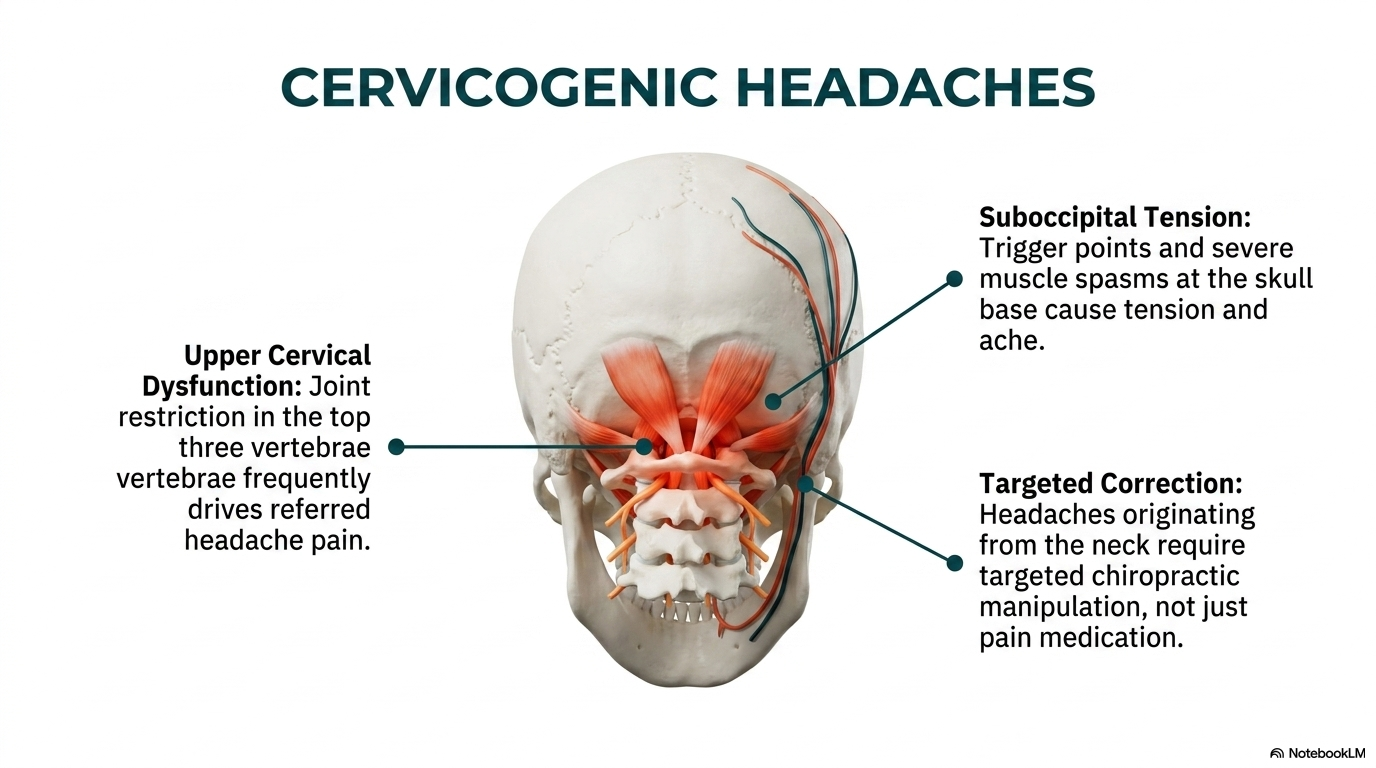
Many recurrent headaches originate in the cervical spine. Cervicogenic headaches arise from irritation of the upper cervical nerve roots (C1, C2, C3) and the trigeminal nucleus caudalis — a shared pain processing center that explains why cervical dysfunction produces pain felt in the head, eyes, temples, and sinuses.
Tension-type headaches — the most common headache type — are frequently driven by suboccipital muscle hypertonicity, upper cervical joint restriction, and forward head posture that compresses the C0-C1 articulation. These are mechanical problems with mechanical solutions, not chemical imbalances that require long-term medication.
Patients with post-concussion syndrome, post-whiplash headaches, and chronic daily headaches often have identifiable cervical biomechanical dysfunction that is missed on standard neurological workup — and that responds well to targeted chiropractic care.
Our Approach to Headache Care
Upper Cervical Evaluation
We evaluate the upper cervical spine (occiput, C1, C2) — the most common structural source of cervicogenic headaches. Restriction at the atlanto-occipital or atlanto-axial joints directly irritates the suboccipital nerve complex and produces referred head pain.
Cervical Adjustments
Targeted mobilization of restricted upper and mid-cervical segments reduces the afferent barrage driving referred head pain. Many patients experience significant headache reduction within the first 2-4 visits.
Postural and Mechanical Correction
Forward head posture increases compressive load on the upper cervical segments significantly for every inch of forward displacement. Addressing the postural and mechanical drivers prevents recurrence beyond the treatment period.
Spinal Biomechanics Training Applied to Headache Care
Fellowship training in spinal biomechanics and trauma includes deep study of the craniocervical junction — the mechanical interface between the skull and cervical spine where most cervicogenic headaches originate. This training gives Drs. McClean diagnostic tools not available to general practitioners for identifying cervical headache sources.
When headaches suggest vascular or intracranial pathology, appropriate neurological screening and referral protocols are applied immediately. Patient safety and accurate diagnosis always come first.
Frequently Asked Questions
How do I know if my headaches are coming from my neck?
Key indicators of cervicogenic headaches: pain begins in the neck or base of skull and radiates to the head; headache worsens with certain neck positions or sustained posture; you have associated neck stiffness or restricted range of motion; headaches began or worsened after a neck injury. Diagnostic nerve blocks can confirm the diagnosis definitively.
Can chiropractic care replace my headache medication?
For cervicogenic and tension-type headaches, many patients reduce or eliminate medication reliance after successful treatment of the underlying cervical cause. We do not manage your medications — that is your prescribing physician’s role — but addressing the structural source often makes long-term medication unnecessary.
What types of headaches won’t respond to chiropractic care?
Migraines with vascular or cortical spreading depression mechanisms, headaches from intracranial pathology (tumors, aneurysms), cluster headaches, and headaches from systemic conditions require different management pathways. We screen for these at evaluation and refer appropriately.
Clinical Evidence
Bryans et al., 2011
Evidence-based guidelines from the Journal of Manipulative and Physiological Therapeutics found strong evidence supporting spinal manipulation for cervicogenic headaches and moderate evidence for tension-type headaches — recommending it as a primary treatment alongside multimodal care for both headache types.
Nilsson et al., 1997
A randomized controlled trial compared spinal manipulation to laser (placebo) in patients with cervicogenic headache. The manipulation group showed significantly greater reduction in headache intensity, frequency, and duration at 12 weeks — with no significant improvement in the control group.
Boline et al., 1995
A head-to-head RCT comparing spinal manipulation to amitriptyline (a common headache medication) for chronic tension-type headaches found equivalent improvement during the treatment period — but only the spinal manipulation group maintained benefits after treatment ended, while the medication group returned to baseline.
References
- Bryans R, et al. Evidence-based guidelines for the chiropractic treatment of adults with headache. J Manipulative Physiol Ther. 2011;34(5):274-289.
- Nilsson N, Christensen HW, Hartvigsen J. The effect of spinal manipulation in the treatment of cervicogenic headache. J Manipulative Physiol Ther. 1997;20(5):326-330.
- Boline PD, et al. Spinal manipulation vs amitriptyline for the treatment of chronic tension-type headaches. J Manipulative Physiol Ther. 1995;18(3):148-154.
Schedule Your Consultation Today
Fellowship-trained spine specialists serving Provo and all of Utah County.
Frequently Asked Questions
Can a chiropractor help headaches?
Yes, particularly headaches that start from the joints and muscles of the upper neck. Restoring normal neck motion often reduces how often and how hard they hit.
How do I know if my headache comes from my neck?
Neck-related headaches often start at the base of the skull, get worse with certain neck positions, and come with neck stiffness. Our exam helps tell them apart from other types.
Are headaches after a car accident normal?
They are common after whiplash. The same neck structures injured in a crash can refer pain into the head. These respond well to care aimed at the neck.
How long until headaches improve with care?
Many patients notice fewer headaches within a few weeks. The cause and history shape the timeline, which we track from visit to visit.
When should a headache be checked right away?
A sudden, severe headache, or one with vision changes, weakness, or confusion, needs urgent medical care. We help you know the difference.