Two Good Treatments. One Sequence Problem.
Physical therapists are skilled clinicians. The best ones understand spinal mechanics well, use manual techniques, and do far more than hand a patient a printout of exercises. Chiropractic care and physical therapy work together effectively in many spine practices, including ours. Referrals move in both directions.
Still, there is a sequencing problem in how herniated disc patients are typically managed that is worth discussing honestly. Most patients with a disc herniation receive a physical therapy referral before anyone has assessed what is happening mechanically at the level of the spine. The physical therapy may be excellent. It may still be the wrong intervention at that stage of the problem, not because of any failure on the therapist’s part, but because it does not address what is driving the disc problem in the first place.
Understanding why requires a look at how a disc herniation actually develops and what treatment can do to the mechanical environment around it.
What Drives A Disc Herniation
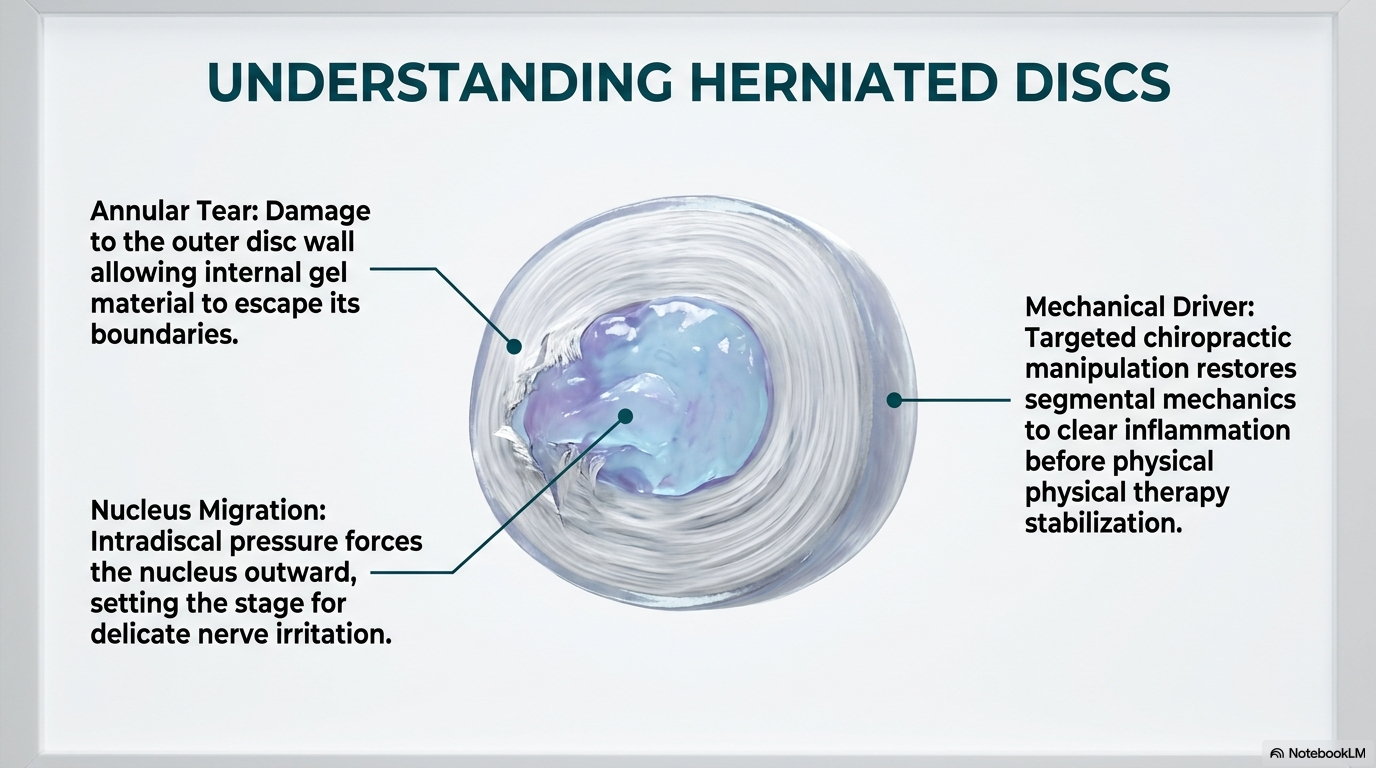
The intervertebral disc sits between two vertebral bodies and acts as both a shock absorber and a pivot point for spinal movement. The outer ring, called the annulus fibrosus, is made of layered collagen fibers oriented at alternating angles to resist compression, rotation, and shear. The inner core, the nucleus pulposus, is a hydrated gel that distributes compressive load evenly when the disc mechanics are working correctly.
A disc herniation occurs when the nucleus migrates through a tear or weakness in the annular fibers and contacts the spinal cord or a nerve root. The immediate result is both mechanical (pressure on neural tissue) and chemical. The nucleus contains inflammatory proteins that irritate the nerve even before significant compression is present.
What allows this to happen is almost always a problem with how the segment is moving. When a spinal segment loses its normal motion pattern, whether through restriction, hypermobility, or misalignment, the disc absorbs load unevenly. Specific regions of the annulus are stressed repeatedly in directions they are not built to handle. Over time, those fibers fatigue and fail. The herniation is the end result of a mechanical fault that may have been present long before the disc gave way.
This is the problem that needs to be addressed first.
How Manipulation Helps The Disc: Several Mechanisms At Once
Spinal manipulation restores motion to a restricted or dysfunctional segment. That sounds simple. The physiological effects are not.
When a chiropractor applies a controlled adjustment to a spinal segment, several things happen simultaneously. First, the facet joints at that level are mobilized through a range they had not been achieving, releasing adhesions that form in joint capsules during periods of restricted movement. Second, the mechanoreceptors in the joint capsule (highly specialized nerve endings that communicate position and movement information to the brain) resume normal signaling. The brain’s map of where the spine is and how it is moving is updated with accurate information, and the protective muscle guarding that was holding the segment rigid begins to release.
Third, and this is often overlooked in the conversation about disc herniations, manipulation creates a pressure change within the disc itself. The brief distraction force applied during an adjustment changes the hydraulic pressure in the nucleus, which can help move nuclear material away from the nerve root. This is not a guaranteed outcome, and it is not the primary mechanism, but it contributes to why many patients with radiculopathy from disc herniation feel relief from manipulation that they do not get from rest or exercise.
Fourth, manipulation stimulates local blood flow to the treated area. The spinal joints, ligaments, and surrounding soft tissues receive increased circulation following manipulation. For a disc that is inflamed, and most symptomatic disc herniations involve local inflammatory activity, this increased blood flow helps clear the inflammatory byproducts that sensitize the nerve root. Research by Teodorczyk-Injeyan and colleagues found that spinal manipulation reduces the production of pro-inflammatory cytokines, the chemical messengers that sustain the inflammatory response at the injured site. This anti-inflammatory effect is a mechanism that exercise does not replicate in the same way.
Fifth, manipulation activates pain-inhibitory pathways in the spinal cord and brain. The gate control theory of pain, first described by Melzack and Wall, holds that the activation of large-diameter sensory nerve fibers, which manipulation does, inhibits the transmission of pain signals through smaller pain-conducting fibers. Separately, manipulation has been shown to trigger the release of endorphins and other endogenous opioids. These neurological effects explain why patients often report immediate pain reduction following an adjustment that persists well beyond the duration of any mechanical change that could have occurred during the treatment.
What Physical Therapy Adds: After The Mechanical Driver Is Addressed
None of the above means physical therapy has no role in herniated disc management. It has a critical one, at the right stage.
Once the dysfunctional segment is moving normally, once the disc’s mechanical environment has improved, once the acute inflammation has settled, the spine needs to be stabilized and rehabilitated. This is exactly what physical therapy is built to do. Specific stabilization exercises targeting the deep segmental muscles, particularly the multifidus and transversus abdominis, help prevent recurrence by building the active support system around segments that are now moving correctly. Work by Hides, Richardson, and Jull demonstrated that these muscles do not recover spontaneously after a spine episode, and that targeted rehabilitation reduces recurrence rates significantly compared to rest or general exercise alone.
Progressive functional loading, postural re-education, work conditioning, and movement retraining all have value. Physical therapists are often the right people to deliver these interventions. The question is not whether these interventions are useful. It is whether they are appropriate in the early phase of a disc herniation before the mechanical driver has been treated.
Applying a progressive loading program to a spine that is still mechanically dysfunctional can increase intradiscal pressure, which Nachemson’s pressure studies quantified precisely, without correcting the segmental fault driving the herniation. For patients with acute disc herniations and active radiculopathy, this can extend the inflammatory phase and delay recovery.
The Logical Sequence
The appropriate pathway for most herniated disc patients without neurological emergency is this. Start with a biomechanical assessment of the spine that evaluates how each segment is moving, where the mechanical fault is, and what the imaging actually shows in context. Initiate manipulation to restore normal segmental mechanics, reduce joint inflammation, improve local blood flow, and create a better mechanical environment for disc recovery. Monitor the clinical response, which is itself diagnostic information. When the acute phase has resolved, transition to stabilization and functional rehabilitation, with physical therapy as a collaborative partner in that phase.
This is not a competition between professions. It is a logical ordering of two good treatments based on what each one actually does and when the spine is ready for it.
The Patients We See Most Often
The patients who arrive at our office with the longest recovery ahead are almost always the ones who spent two or three months in physical therapy before anyone looked at how the spine was actually moving. By that point, the inflammation has become more established, the segmental mechanics have adapted around the dysfunction, and the central nervous system has begun to reorganize around a pain pattern. These patients still do well with chiropractic care, but the course is longer.
A patient who receives a proper biomechanical evaluation early, ideally within the first few weeks of a disc herniation, and who receives manipulation to address the mechanical driver before undertaking a rehabilitation program is in a substantially better position at six months than one who followed the standard referral pathway in reverse.
If you have a disc herniation and have been told that physical therapy is your next step, it may well be. It is also worth having a structural evaluation of your spine first to determine whether there is a mechanical driver that should be addressed before the rehabilitation phase begins. That is a conversation worth having before committing to a course of care.
References
- Santilli V, Beghi E, Finucci S. Chiropractic manipulation in the treatment of acute back pain and sciatica with disc protrusion: a randomized double-blind clinical trial of active and simulated spinal manipulations. Spine J. 2006;6(2):131-137.
- Nachemson A. Disc pressure measurements. Spine. 1981;6(1):93-97.
- Teodorczyk-Injeyan JA, Injeyan HS, Ruegg R. Spinal manipulative therapy reduces inflammatory cytokines but not substance P production in normal subjects. J Manipulative Physiol Ther. 2006;29(1):14-21.
- Hides JA, Richardson CA, Jull GA. Multifidus muscle recovery is not automatic after resolution of acute, first-episode low back pain. Spine. 1996;21(23):2763-2769.
- Leemann S, Peterson CK, Schmid C, Anklin B, Humphreys BK. Outcomes of acute and chronic patients with magnetic resonance imaging-confirmed symptomatic lumbar disc herniations receiving high-velocity, low-amplitude spinal manipulative therapy. J Manipulative Physiol Ther. 2014;37(3):155-163.
- Melzack R, Wall PD. Pain mechanisms: a new theory. Science. 1965;150(3699):971-979.
- Panjabi MM. The stabilizing system of the spine. Part I. Function, dysfunction, adaptation, and enhancement. J Spinal Disord. 1992;5(4):383-389.
Have a disc herniation diagnosis? Find out what is happening mechanically first.
A biomechanical spine evaluation tells you what is driving your disc problem and whether the mechanical driver has been addressed. Call 801-373-1035 to schedule.