Many shoulder problems start in the neck and upper back - and never get treated there.
Why Your Shoulder Pain Might Not Be a Shoulder Problem
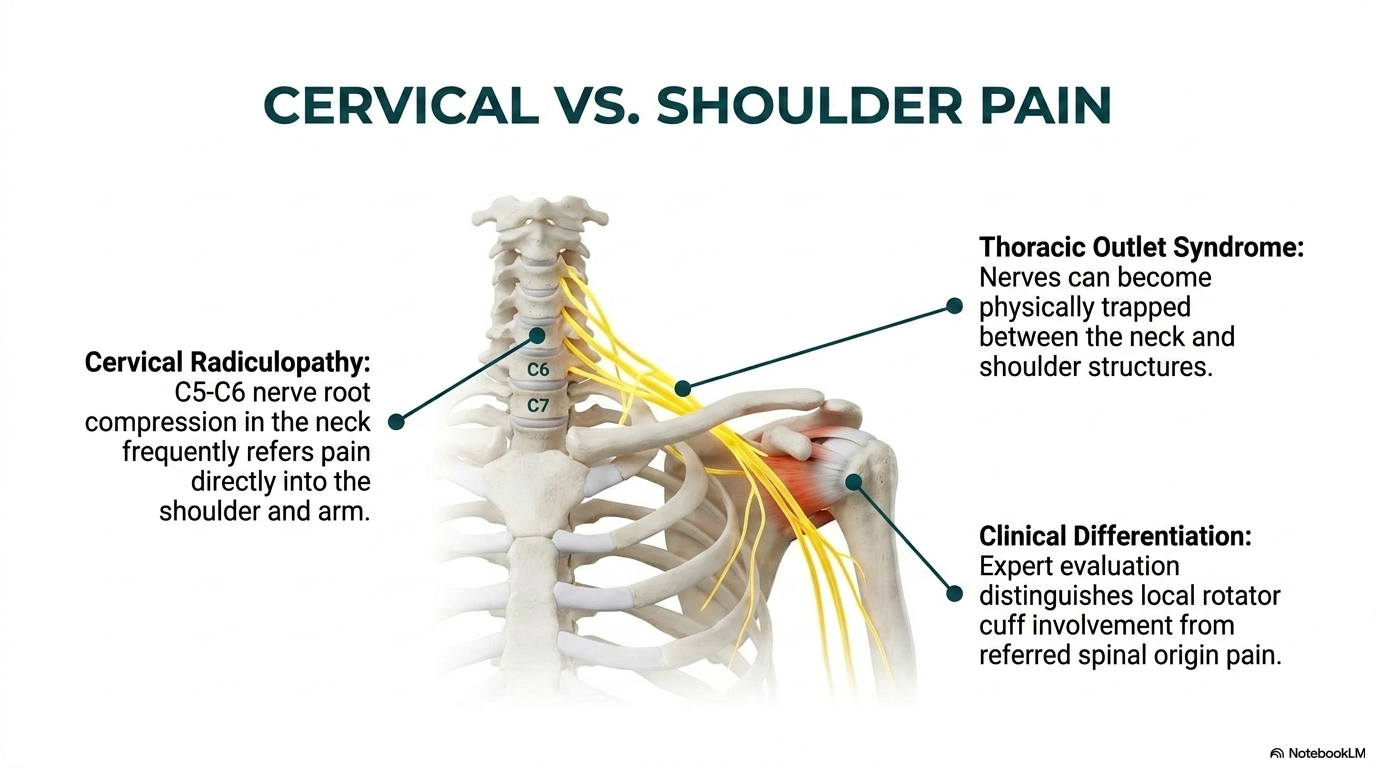
The nerves that control your shoulder and arm originate in your lower cervical spine – C5, C6, C7. When those levels are compressed, irritated, or restricted, the pain, weakness, or numbness shows up in your shoulder or arm. Treating only the shoulder misses the root cause entirely. Our evaluation always includes the full cervical and thoracic spine to determine where your shoulder pain is actually coming from.
Shoulder & Upper Body Conditions We Treat
Rotator Cuff Strain
Soft-tissue injury to the rotator cuff often occurs alongside cervical dysfunction. We treat both to restore full shoulder mechanics.
Shoulder Impingement
When the shoulder joint loses proper mechanics – often driven by thoracic kyphosis – tendons get pinched. Restoring spinal alignment removes the impingement.
Thoracic Outlet Syndrome
Compression of nerves and blood vessels between the collarbone and first rib causes arm pain, numbness, and weakness. The upper thoracic spine is almost always involved.
Neck-Related Shoulder Pain
C5-C7 nerve root involvement refers pain into the shoulder, upper arm, and between the shoulder blades. Looks like a shoulder problem – is actually spinal.
Post-Accident Shoulder Injuries
Whiplash often injures the acromioclavicular joint and rotator cuff alongside the cervical spine. We evaluate both simultaneously.
Frozen Shoulder (Adhesive Capsulitis)
While primarily a shoulder condition, cervical restriction and thoracic dysfunction contribute to the pain cycle of frozen shoulder. Chiropractic care helps restore mobility faster.
Fellowship-Trained. Rarely Matched.
Our doctors hold the FSBT designation – Fellowship in Spinal Biomechanics and Trauma. This post-doctoral training is pursued by a small fraction of chiropractors and equips our team with advanced expertise in spinal imaging, ligament injury assessment, and trauma biomechanics. You get a level of analysis that most chiropractic clinics simply cannot offer.
Frequently Asked Questions
How do you determine if my shoulder pain is spinal or local?
Through a thorough orthopedic and neurological examination plus review of any imaging. We look at the full picture – cervical spine, thoracic spine, and shoulder joint mechanics.
Do I need an MRI for shoulder pain?
Not always. If you already have imaging, we can review it. If you do not, we will determine whether imaging is needed based on your exam findings.
Can chiropractic help after shoulder surgery?
Yes. Post-surgical care often focuses on restoring the surrounding spinal mechanics that contributed to the original problem and supporting full recovery.
How long until I see improvement?
Many patients notice improvement within the first few visits. Complex or long-standing cases take longer. We will give you a realistic timeline after your evaluation.
Ready to Get Relief?
Call us today or request an appointment online. Same-day appointments are often available.
How we evaluate shoulder pain
Most shoulder pain isn't a shoulder problem
- Cervical spine dysfunction referring pain into the shoulder
- Rib and thoracic restriction affecting shoulder mechanics
- Postural compensations loading the rotator cuff
- Neural tension from a pinched cervical nerve
How we find the real source
- Full cervical-thoracic-shoulder biomechanical exam
- Motion X-ray of the neck when referred pain is suspected
- Shoulder orthopedic testing to rule in/out rotator cuff
- MRI referral and correlation when needed
- Functional movement assessment for overhead athletes
What our patients say
“I had tingling and numbness in one arm and back. Dr. Matt McClean did X-rays and ordered an MRI and found an impinged nerve. He carefully adjusted and his staff were very methodical about exercises and treatment.”
. Bobbi K., Google review
“I have had upper back/neck/shoulder issues for years and finally decided to try these guys. Not only have I felt way better physically, but I also love coming in to see them.”
. Lance S., Google review
Shoulder pain FAQ
Specific orthopedic tests, a careful history, cervical motion exam, and often motion X-ray. True rotator cuff problems and referred cervical pain look different on examination. You just have to actually do the exam.
Partial-thickness tears often respond well to conservative care. Full-thickness tears usually need surgical evaluation. We’ll be straight with you after the exam and imaging.
No. Long-standing shoulder dysfunction often has layered causes (posture, cervical, rotator cuff, scapular mechanics). We unpack those methodically and usually make meaningful progress even on “chronic” cases.
Instrument-assisted soft tissue mobilization, yes. We coordinate with other providers for dry needling when it’s indicated.
We treat adhesive capsulitis with a combination of graded mobilization, cold laser, stretching, and strengthening through the phases. It’s slow by nature but responds well to consistent, appropriate care.
Surgical-grade tears, labral tears that are blocking function, and shoulders that aren’t responding to 6-8 weeks of appropriate conservative care.
Shoulder pain that won't quit? Let's find the real source.
Same-week appointments available. Insurance accepted. Let’s get you a real evaluation and a plan.
McClean Chiropractic · 385 N 500 W, Provo UT 84601
Also consider. Prolozone injections
For chronic shoulder pain. Rotator cuff irritation, labral strain, and shoulder arthritis. prolozone injections can be a powerful adjunct to chiropractic and soft-tissue care. Prolozone combines homeopathics with medical-grade ozone to support regeneration inside the joint. Learn more about prolozone therapy.
Clinical Evidence
BRANTINGHAM JW, ET AL., 2011
Manipulative therapy for shoulder pain and disorders: systematic review expansion confirms efficacy of manual care for shoulder dysfunction.
BERGMAN GJ, ET AL., 2004
Manipulative therapy in addition to usual medical care for patients with shoulder dysfunction and pain produced significantly better short-term outcomes.
PRIBICEVIC M, POLLARD H., 2005
A multi-modal treatment approach for the shoulder including chiropractic manipulation demonstrated positive outcomes across a case series.
References
- Brantingham JW, et al. Manipulative therapy for shoulder pain and disorders: expansion of a systematic review. J Manipulative Physiol Ther. 2011;34(5):314-46.
- Bergman GJ, et al. Manipulative therapy in addition to usual medical care for patients with shoulder dysfunction and pain. Ann Intern Med. 2004;141(6):432-9.
- Pribicevic M, Pollard H. A multi-modal treatment approach for the shoulder: a 4 patient case series. Chiropr Osteopat. 2005;13:20.
Related at McClean Chiropractic