Back Pain Treatment in Provo, Utah
Structural diagnosis and evidence-based spinal care for lasting low back pain relief.
Yes, chiropractic care helps most back pain. Our fellowship-trained Provo doctors use motion X-ray and a thorough exam to find the mechanical cause, then build a plan around it.
Low Back Pain: Finding the Source
Low back pain is the leading cause of disability worldwide and the most common reason for lost workdays in the United States. Despite its prevalence, it is frequently mismanaged — treated as a symptom rather than addressed at its structural source.
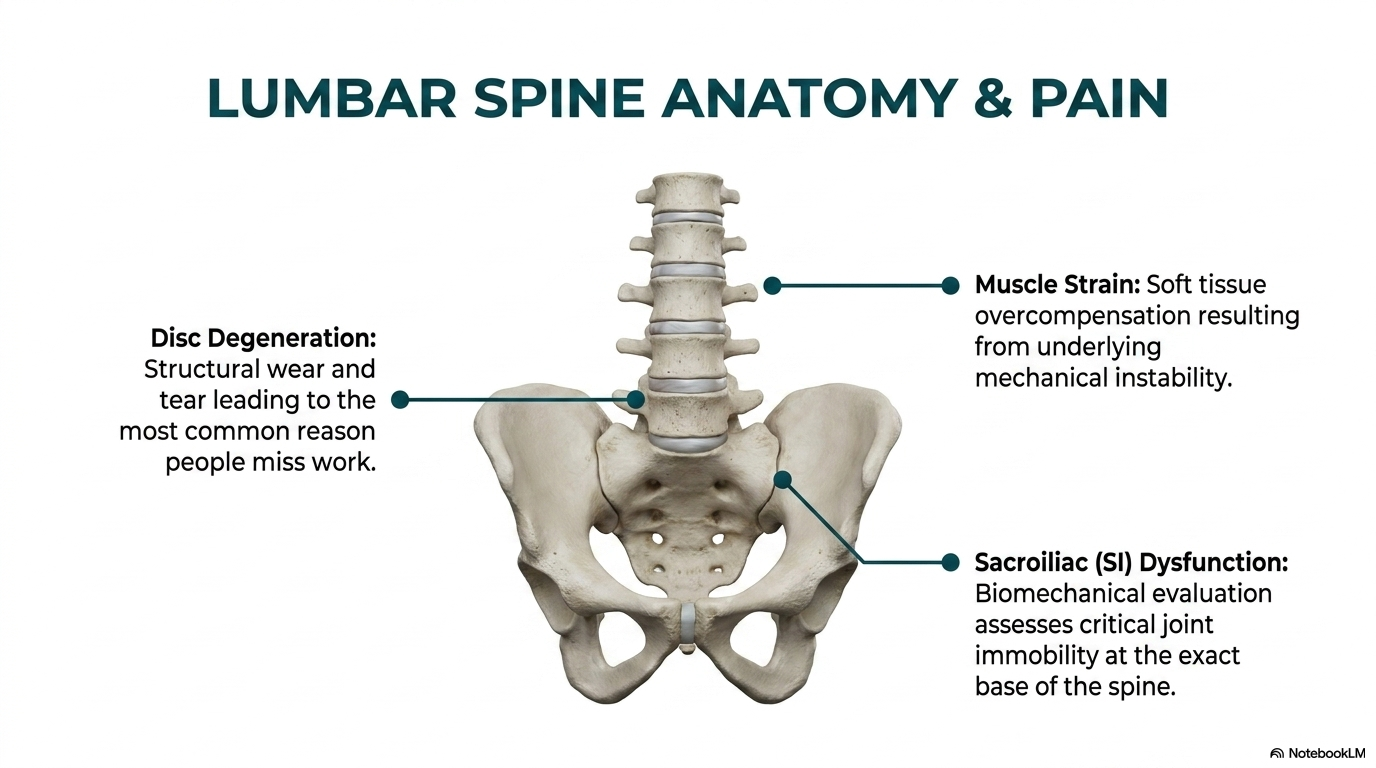
Mechanical low back pain arises from specific spinal structures: intervertebral discs, facet joints, ligaments, sacroiliac joints, and the muscles and fascia supporting the lumbar spine. Identifying which structure is generating pain — and why — determines whether treatment will succeed. Generic protocols applied without structural diagnosis produce temporary, incomplete results.
Our Approach to Low Back Pain
Biomechanical Spine Analysis
Full-spine X-ray with angular measurements identifies structural drift, compensatory patterns, and the specific segmental levels driving mechanical pain. Motion X-ray shows which joints are restricted or unstable under load.
Spinal Manipulation
High-velocity, low-amplitude adjustments at restricted lumbar segments restore normal joint motion, normalize facet joint mechanics, and interrupt the neurological pain amplification cycles that sustain chronic low back pain.
Spinal Decompression
Spinal decompression is an established conservative treatment for disc-related symptoms with clinical support in the peer-reviewed literature. It is applied based on your specific examination findings and imaging, as part of an individualized care plan. Sessions run approximately 15 minutes.
Fellowship-Trained Low Back Specialists
Most chiropractors treat symptoms. Fellowship-trained spinal biomechanics specialists treat the underlying mechanical cause. Drs. McClean hold the FSBT designation — post-doctoral training in biomechanical spine analysis, MRI interpretation, and structural treatment protocols not taught in standard chiropractic programs.
This level of training means we can accurately differentiate disc-mediated pain from facet pain from sacroiliac dysfunction — and apply the right treatment for the right diagnosis, rather than using the same approach for everyone.
Frequently Asked Questions
My MRI looks normal but my back still hurts. Why?
MRI is an excellent anatomical tool but a poor functional tool. It cannot show which segments are hypomobile or unstable, how your spine loads and moves under normal conditions, or the status of small ligaments that stabilize individual vertebral joints. Motion X-ray fills many of these gaps — and many clinically significant problems are invisible on standard MRI.
Should I try chiropractic before considering surgery?
Yes, in most cases. Clinical guidelines from multiple medical organizations recommend conservative treatment — including spinal manipulation — before surgical intervention for non-emergency low back pain. Surgery for back pain carries significant risks and has variable outcomes; a thorough conservative trial first is appropriate medicine.
I’ve had back pain for years. Is it too late to improve?
Chronic low back pain often responds well to care that addresses the underlying mechanical driver. Even patients with long-standing pain, prior surgery, or degenerative changes frequently achieve significant improvement when structural diagnosis guides treatment.
Clinical Evidence
Rubinstein et al., 2011
A Cochrane systematic review (n=2,028) found spinal manipulative therapy statistically and clinically superior to sham manipulation for chronic low back pain in the short, intermediate, and long term — with effect sizes comparable to other recommended treatments including NSAIDs and supervised exercise.
Goertz et al., 2013
A randomized trial published in Spine found that adding chiropractic manipulative therapy to standard medical care produced significantly greater improvement in low back pain and disability at 6 weeks compared to standard care alone — with benefits maintained at 52-week follow-up.
Chou et al., 2007
The American College of Physicians and American Pain Society joint clinical practice guideline (Annals of Internal Medicine) recommends spinal manipulation as a first-line treatment option for acute and subacute low back pain, alongside supervised exercise and NSAIDs — and ahead of opioids.
References
- Rubinstein SM, et al. Spinal manipulative therapy for chronic low-back pain. Cochrane Database Syst Rev. 2011;(2):CD008112.
- Goertz CM, et al. Adding chiropractic manipulative therapy to standard medical care for patients with acute low back pain. Spine. 2013;38(8):627-634.
- Chou R, et al. Diagnosis and treatment of low back pain: a joint clinical practice guideline. Ann Intern Med. 2007;147(7):478-491.
Schedule Your Consultation Today
Fellowship-trained spine specialists serving Provo and all of Utah County.
More From Our Spine Education Library
Articles from our fellowship-trained doctors on the topics above:
- Why Some Spines Age Well and Others Do Not
- Catching Patients Before They Become Chronic
- Chiropractic Care and the Opioid Crisis: What the Research Actually Shows
- Why Telling a Patient to Move More Is Not Enough
- Your Spine Is Not Just a Structure. It Is a Sensory System.
- Why You Cannot Exercise Your Way Out of a Spine Problem
- What Is Actually Happening When Your Spine “Goes Out”
Frequently Asked Questions
Can a chiropractor help lower back pain?
Yes. Most low back pain is mechanical, meaning it comes from joints, discs, or muscles that are not working well together. Restoring normal motion relieves the pain and lowers the chance it returns.
How long until my back pain gets better?
Many people improve within the first few weeks. The timeline depends on the cause and how long it has been there, which is why we measure your progress rather than guess.
Is it better to rest or move with back pain?
Gentle movement usually beats bed rest for most back pain. The right kind of movement depends on what is driving your pain, so we guide it rather than just telling you to move more.
What if my MRI looks normal but my back still hurts?
That is common. A scan is a snapshot and can miss how your spine moves. Motion X-ray and a hands-on exam often find the cause a static image cannot.
When should back pain be checked by a doctor?
If you have leg weakness, numbness, loss of bladder or bowel control, or pain after a fall or crash, get seen promptly. We evaluate and refer out when needed.
Stop the flare-up cycle for good
Back pain that returns every few months usually means the spine’s stabilizing system never fully recovered. Our computerized spine stability program tests your stability, left/right symmetry, and endurance on load-cell instrumented machines, then retrains what the testing finds.