Sciatica or Leg Pain?
Get to the cause, not just the symptom · same-day visits available.
📞 Tap to Call: (801) 373-1035 ★ 4.7 from 250+ Utah County patients · Fellowship-trained spine specialistsRequest a Callback
Tell us how to reach you - we'll call you back fast. No cost, no obligation.
Prefer to talk now? Call (801) 373-1035.
Thanks - we've got it!
Our team will call you back shortly. Need us now? Call (801) 373-1035.
Sciatica Treatment in Provo, Utah
Identifying and treating the mechanical cause of sciatic nerve pain — not just masking symptoms.
Most sciatica can be relieved without surgery. For the majority of patients, identifying exactly which nerve root is compressed – and treating that cause with spinal decompression and targeted care – relieves sciatic leg pain within a few weeks. The first step is an accurate diagnosis that separates true sciatica from the conditions that mimic it.
What Is Sciatica?
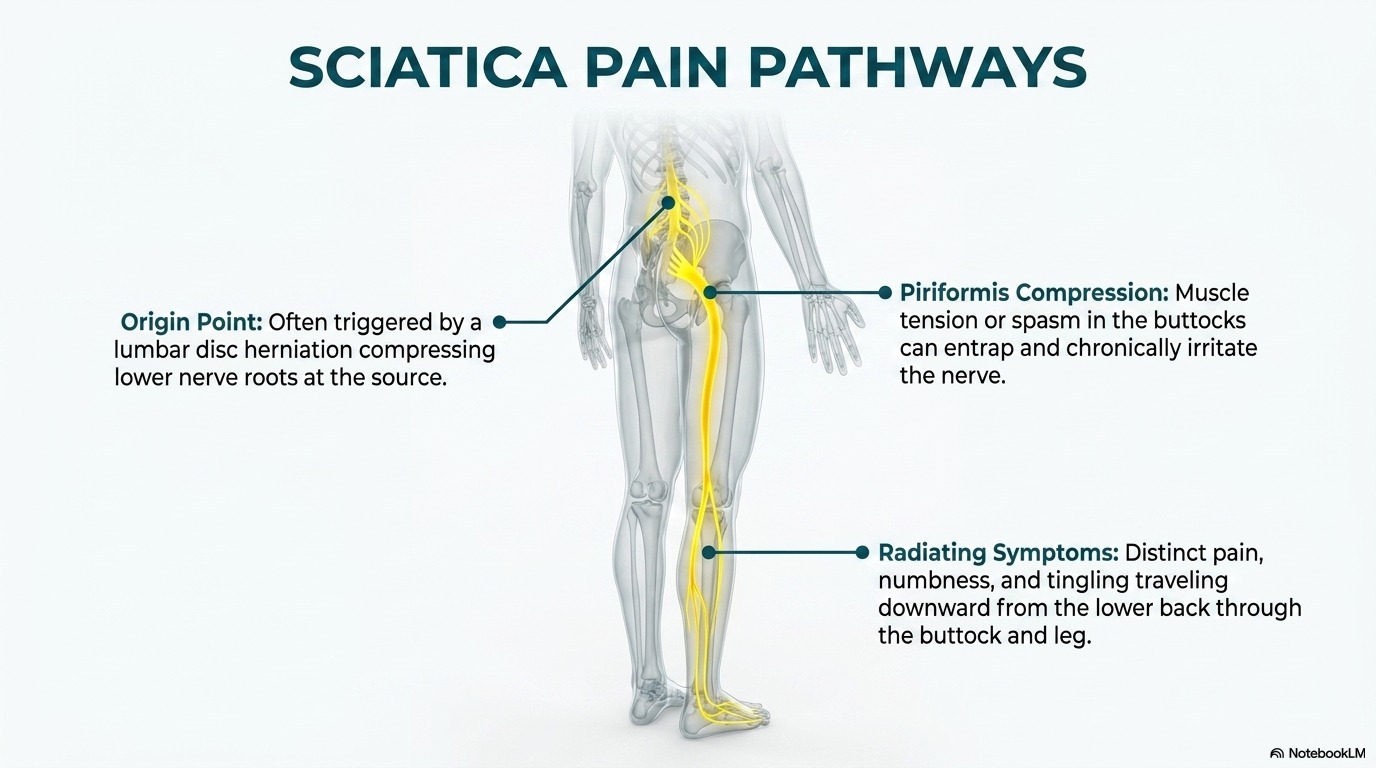
Sciatica is pain that travels along the path of the sciatic nerve — from the lower back through the hip, buttock, and down the leg, often reaching the foot. It typically affects one side of the body and ranges from a mild ache to a sharp, burning sensation or electric shock-like pain.
True sciatica is caused by compression or irritation of one or more nerve roots that form the sciatic nerve (L4, L5, S1, S2, S3). Common causes include disc herniation, bone spurs, spinal stenosis, piriformis syndrome, and sacroiliac joint dysfunction. Accurate diagnosis of the compressive source is essential — treatment that targets the wrong structure will fail.
How We Treat Sciatica
Nerve Root Identification
We use full-spine X-ray analysis, motion fluoroscopy, and clinical neurological testing to identify which nerve root(s) are involved and what structure is compressing them — disc, facet, or ligament.
Spinal Decompression
Spinal decompression is an established conservative treatment for disc-related symptoms with clinical support in the peer-reviewed literature. It is applied based on your specific examination findings and imaging, as part of an individualized care plan. Sessions run approximately 15 minutes.
Targeted Spinal Adjustments
Segmental adjustments at the affected lumbar and sacral levels restore normal motion, reduce facet-mediated compression, and interrupt the neurological feedback loops sustaining sciatic pain patterns.
Spine Specialists. Not Generalists.
The FSBT (Fellowship in Spinal Biomechanics and Trauma) designation requires post-doctoral training in MRI interpretation, advanced biomechanical analysis, and trauma mechanisms — skills directly applicable to diagnosing the structural causes of sciatic nerve compression.
Drs. McClean have maintained direct working relationships with Utah County spine surgeons and MRI facilities since 1999. When surgery or injection referral is indicated, they coordinate directly with the appropriate specialist.
Frequently Asked Questions
Can a chiropractor help with sciatica?
Yes – for most patients, sciatica responds well to non-surgical chiropractic care once the true source of the nerve compression is identified. Our fellowship-trained doctors pinpoint which nerve root is involved and what is compressing it – disc, facet, or ligament – then target that cause directly with spinal decompression and specific treatment rather than only easing the symptom.
How long does sciatica take to heal?
Most cases of sciatica improve within a few weeks of starting appropriate conservative care, and many patients feel meaningful relief in the first several visits. The timeline depends on what is compressing the nerve and how long it has been present, which is why an accurate diagnosis up front matters more than any fixed number of sessions.
Is my leg pain definitely sciatica?
Not necessarily. Peripheral vascular disease, hip joint pathology, piriformis syndrome, and referred pain from sacroiliac joints can all produce leg pain resembling sciatica. Accurate diagnosis matters – we use orthopedic testing, neurological evaluation, and imaging to identify the true source.
Do I need an MRI to get treated?
No, but imaging often helps confirm the diagnosis and guide treatment. If you already have MRI or X-ray images, bring them. We can also order imaging and have direct relationships with local MRI facilities in Utah County.
When should sciatica be treated as an emergency?
If you experience loss of bladder or bowel control, progressive leg weakness, or saddle anesthesia (numbness in the groin and inner thighs), seek emergency care immediately – these may indicate cauda equina syndrome, a surgical emergency.
Clinical Evidence
Santilli et al., 2006
A randomized controlled trial published in Spine Journal compared high-velocity spinal manipulation to simulated manipulation in patients with acute sciatica and disc protrusion. The manipulation group showed significantly greater pain reduction and faster return to normal activity over a 6-month follow-up period.
Weinstein et al., 2006
The SPORT trial (JAMA, 2006) — one of the largest spine surgery RCTs ever conducted — found that patients with disc herniation and radiculopathy who opted for conservative treatment showed substantial improvement comparable to surgery at 2-year follow-up, supporting non-surgical care as first-line treatment.
Saal & Saal, 1989
In patients with lumbar disc herniation and radiating leg pain (including sciatica), aggressive non-operative rehabilitation produced 92% good-to-excellent outcomes, with 87% returning to their previous occupation — results that remain a benchmark for non-surgical disc care.
References
- Santilli V, Beghi E, Finucci S. Chiropractic manipulation in the treatment of acute back pain and sciatica with disc protrusion. Spine J. 2006;6(2):131-137.
- Weinstein JN, et al. Surgical vs nonoperative treatment for lumbar disc herniation: the Spine Patient Outcomes Research Trial (SPORT). JAMA. 2006;296(20):2441-2450.
- Saal JA, Saal JS. Nonoperative treatment of herniated lumbar intervertebral disc with radiculopathy. Spine. 1989;14(4):431-437.
Schedule Your Consultation Today
Fellowship-trained spine specialists serving Provo and all of Utah County.
A complete non-surgical option for disc injuries
Our Disc Recovery Program combines spinal decompression and Class IV laser therapy, guided by fellowship-trained doctors who read your MRI themselves. If your sciatica is coming from a disc problem, this is the structured way to treat it without surgery.
Related Spine Conditions We Treat
Fellowship-trained care across Provo & Utah County. Explore related conditions:
Tired of sciatica that keeps coming back?
Recurring sciatica is usually a spinal control problem, not just a nerve problem. Our computerized spine stability program measures the left/right imbalances and early fatigue that trigger flare-ups, then retrains your spine with force-feedback machines you will not find at any other clinic in Utah County.
More From Our Spine Education Library
Articles from our fellowship-trained doctors on the topics above: