Non-Surgical Spinal Decompression
Provo, Utah — MRI-Confirmed Results. Fellowship-Level Care.
Spinal decompression is a non-surgical, computer-guided traction therapy for disc-related conditions. At McClean Chiropractic, we apply decompression as part of an individualized care plan guided by your examination findings and imaging — combined with chiropractic manipulation when appropriate.
Spinal decompression is a non-surgical treatment that gently relieves pressure on a herniated or degenerated disc. In Provo, our fellowship-trained doctors use MRI to confirm you are a good candidate first.
What Is Non-Surgical Spinal Decompression?
Non-surgical spinal decompression (NSD) is a computer-controlled motorized traction therapy that differs from the sustained-force traction once used in physical therapy. The distinction matters clinically.
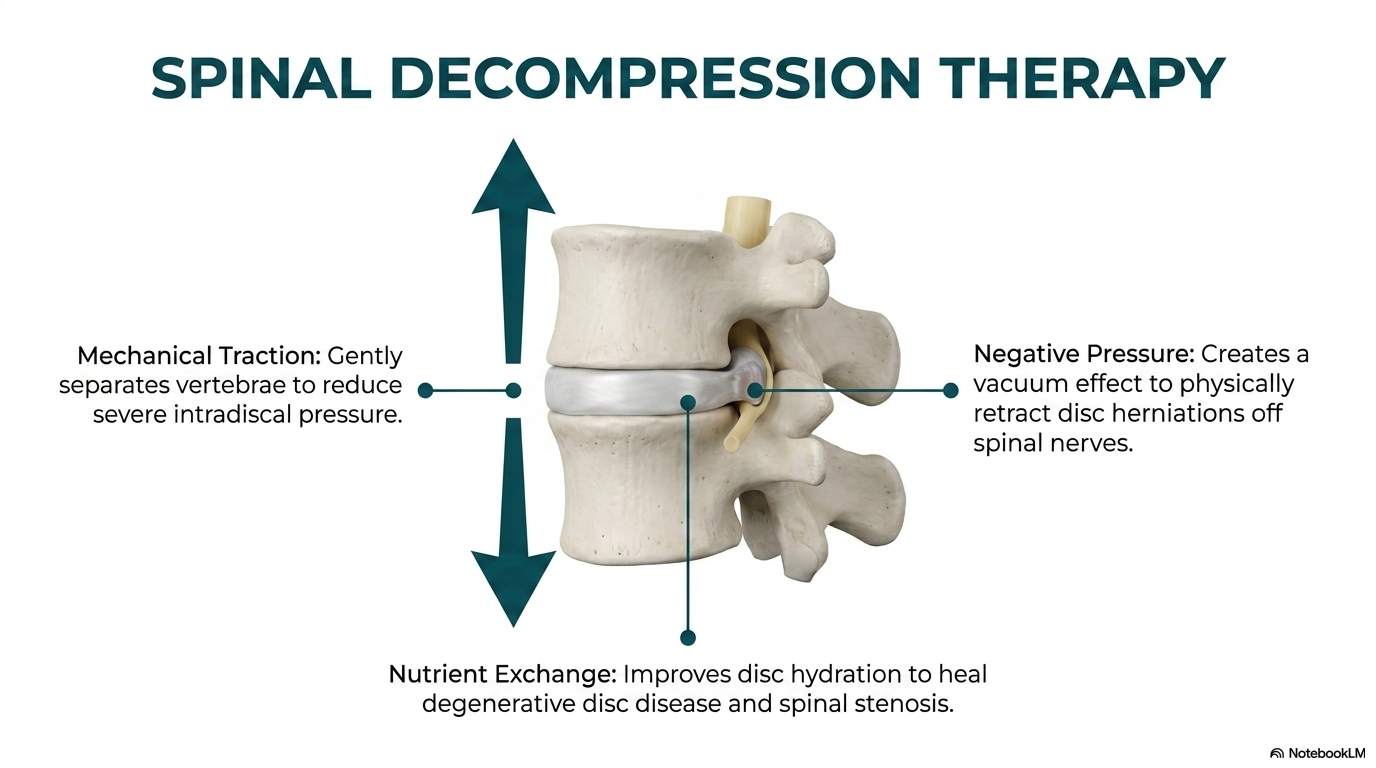
Conventional traction applies a sustained pulling force. The body responds by activating protective muscle guarding — the paraspinal muscles contract against the stretch, which limits how much effect reaches the disc. Non-surgical spinal decompression addresses this through a computerized feedback system. Sensors detect when muscles begin to resist, and the table modulates the tension in a rhythmic pattern that allows greater paraspinal relaxation and more sustained distraction at the lumbar levels.
Clinical studies support NSD as a conservative option for lumbar disc herniation and disc-related radiculopathy. We use decompression as one component of your individualized care plan, determined by your specific examination and imaging findings. Treatment frequency and duration are based on your response to care — there is no fixed protocol applied to every patient.
How Spinal Decompression Works
Computer-Guided Distraction
The therapy uses a computerized feedback system to modulate spinal distraction in a rhythmic pattern — reducing the protective muscle guarding reflex that limits effectiveness with conventional traction. The result is more sustained distraction at the affected disc levels.
Disc Hydration & Fluid Exchange
The intervertebral disc is avascular — it has no direct blood supply and depends on alternating compression and decompression to exchange fluid and nutrients. Degenerated discs have reduced capacity for this exchange. Decompression therapy applies the axial distraction component of this cycle in a controlled, rhythmic manner.
Part of a Clinical Care Plan
Decompression is one tool in a broader clinical approach. At McClean Chiropractic, it is combined with chiropractic manipulation, postural correction, and guidance on activity modification — applied in the combination indicated by your specific examination and imaging findings.
The Evidence: MRI-Confirmed Disc Reduction
A 2024 case series published in the Journal of Contemporary Chiropractic by Dudum and Gatterman is among the most clinically compelling evidence available for non-surgical decompression combined with chiropractic care.
Patients showed MRI-confirmed reduction in disc herniation size after the combined NSD + chiropractic protocol
Range of disc herniation reduction measured by herniation index on follow-up MRI imaging
Patient-reported pain improvement at 2-month follow-up, with full recovery documented at 3–6 months
Treatment protocol duration — 20–30 sessions of NSD combined with chiropractic adjustments and supportive therapies
One patient presented with complete S1 nerve root compression on MRI. Following 8 weeks of NSD and chiropractic care, the follow-up MRI showed visible decompression of the nerve root and 29.5% reduction in disc herniation size — with the nerve root now visible in the subarticular recess where it had previously been obliterated. The patient was pain-free at four-month follow-up.
Source: Dudum JD, Gatterman B. Reduction of the size of a lumbar disc herniation using non-surgical spinal decompression combined with chiropractic care. J Contemp Chiropr. 2024;7:146-155.
Conditions We Treat with Spinal Decompression
Spinal decompression is not a one-size-fits-all treatment. It is most effective when the mechanical driver of the disc problem has been identified and addressed. We use a thorough biomechanical evaluation — including motion X-ray when appropriate — to determine whether decompression is indicated and what disc levels are involved.
Lumbar Disc Herniation
The primary indication for decompression. Effective for herniations with and without sciatica — confirmed herniation on MRI is the strongest predictor of favorable outcome.
Cervical Disc Herniation
Neck disc herniations causing arm pain, numbness, or weakness. Cervical decompression uses a different harness configuration and lower tension but the same negative-pressure mechanism.
Degenerative Disc Disease
Discs that have lost height and hydration respond to the fluid exchange mechanism of decompression. Not a reversal of degeneration, but a meaningful improvement in disc environment and pain reduction.
Spinal Stenosis
For stenosis driven by disc herniation or bulge rather than pure bony overgrowth. Decompression can reduce the disc contribution to foraminal or central canal narrowing.
Sciatica / Radiculopathy
Radiating leg or arm pain from nerve root compression. Decompression addresses the disc source of the compression — often more effectively than anti-inflammatory medication for persistent radiculopathy.
Failed Conservative Care
Patients who have tried physical therapy, medication, or injections without lasting relief. Decompression addresses the disc environment in a way that exercise and anti-inflammatories alone cannot.
Why Manipulation + Decompression Outperforms Decompression Alone
Most decompression centers treat the disc in isolation. We treat the mechanical system the disc lives inside. The distinction is clinically significant.
A disc herniates because the spinal segment it occupies has lost its normal motion pattern. Whether through restriction, hypermobility, or misalignment, an abnormal segment loads the disc unevenly — stressing specific annular fibers in directions they were not designed to handle. Over time, those fibers fail. The herniation is the end result of a mechanical fault that long predates the disc failure itself.
Applying decompression to a spine where the mechanical driver has not been addressed is like pumping up a tire with a bent rim — you can improve pressure temporarily, but the underlying problem that caused the failure is still present. At McClean Chiropractic, manipulation comes first. Chiropractic adjustments restore normal segmental motion, release facet adhesions, normalize mechanoreceptor signaling, and reduce local inflammation at the joint level. Only after the mechanical environment has been restored do we apply decompression to address the disc itself.
The 2024 case series by Dudum and Gatterman used precisely this combined protocol — NSD together with chiropractic adjustments — and documented MRI-confirmed disc reduction in all four patients. No patient in the series underwent surgery. All patients reached 75–90% pain improvement by two months, with complete recovery documented in multiple cases at five to six months.
Good Candidates for Decompression
- MRI-confirmed disc herniation or bulge
- Radicular symptoms (sciatica, arm pain, numbness, tingling)
- Disc herniation that has not responded to PT or medication
- Failed epidural steroid injections
- Degenerative disc disease with persistent pain
- Spinal stenosis with disc contribution
- Seeking a non-surgical alternative before committing to fusion or discectomy
- Want objective MRI review before making a treatment decision
Decompression May Not Be Indicated If:
- Recent vertebral fracture
- Severe osteoporosis with fracture risk
- Active spinal tumor or metastatic disease
- Grade 2+ spondylolisthesis
- Spinal fusion hardware at the involved level (case-by-case evaluation)
- Cauda equina syndrome (surgical emergency)
- Active infection in the spine
We evaluate all cases individually. A prior surgery, hardware, or complex imaging finding does not automatically exclude you — it means a more careful evaluation is needed before treatment begins.
Fellowship-Level Evaluation. Not a Cookie-Cutter Protocol.
Most decompression centers operate from a single protocol: book the evaluation, confirm a disc herniation exists, start decompression. The diagnosis on imaging becomes the treatment decision.
At McClean Chiropractic, the imaging finding is the starting point, not the conclusion. Our doctors hold a Fellowship in Spinal Biomechanics and Trauma (FSBT) — a post-doctoral credential that includes advanced training in MRI interpretation and spinal biomechanics rarely found in chiropractic or medical practice. When you bring us an MRI, we read the actual imaging series — axial, sagittal, and coronal views — not just the radiologist’s report.
We look for: which spinal segment is mechanically dysfunctional, how the disc herniation relates to that dysfunction, whether motion X-ray is needed to evaluate ligament instability, and whether decompression is appropriate at this stage or whether manipulation should precede it. This evaluation determines your actual treatment plan — not a predetermined package.
What a Decompression Session Looks Like
Treatment frequency and duration vary based on your case. Sessions run approximately 15 minutes. We evaluate your response to care and adjust accordingly — there is no fixed number of visits required.
You lie supine (face up) on the decompression table. Adjustable pelvic and thoracic harnesses are positioned around your body. The computerized control system initiates a gentle distraction force — typically starting below therapeutic level and building across the first few sessions as your response is assessed. The table cycles rhythmically between maximum hold and reduced tension, with the hold-to-rest ratio of 1:1 and oscillation adjusting automatically based on muscle feedback sensors.
Most patients feel nothing more than gentle stretching. Many report immediate relief during the session — sometimes the first reduction in leg pain they have had in months. After decompression, we typically perform a chiropractic adjustment at the identified dysfunctional segment to maintain the mechanical correction and reinforce normal motion patterns before the session ends.
Frequently Asked Questions
Is spinal decompression painful?
No. The distraction force is applied gradually and the computerized feedback system prevents it from reaching levels that trigger protective muscle guarding. Most patients find the treatment relaxing and report reduced pain during and immediately after sessions.
How many sessions will I need?
The evidence-based protocol is 20–30 sessions over 8–10 weeks. Some patients experience significant improvement within the first 10–12 sessions. We re-evaluate throughout the course of care and adjust based on your clinical response.
Does insurance cover spinal decompression?
Most insurance plans do not cover non-surgical spinal decompression. We will review your coverage at your initial visit and discuss our self-pay options and payment plans. Many patients compare the cost favorably against the risks and expense of spine surgery.
Can I have decompression if I’ve had spinal surgery?
It depends on the surgery. Patients with prior discectomy (disc removal without fusion) are often good candidates. Patients with fusion hardware require individual evaluation — in some cases decompression can be applied at adjacent levels. We review your imaging and surgical history before making any recommendation.
Can decompression actually shrink a herniated disc?
Yes — MRI evidence confirms this. The 2024 Dudum-Gatterman case series used a standardized herniation index formula to measure disc herniation size on MRI before and after treatment. All four patients showed objective reduction in disc herniation size, with the largest reduction at 29.5%. One patient had complete S1 nerve root compression before treatment; the nerve root was visible and decompressed on the follow-up MRI.
Do I need to bring my MRI?
Yes, if you have one. We read the actual imaging series — not just the report — and this gives us significantly more information about what is happening mechanically at each disc level. If you have a disc herniation diagnosis but no MRI, we can help coordinate imaging through our local Utah County radiology relationships.
What is a Free MRI Review?
We offer a free consultation in which Dr. McClean reviews your existing spine MRI and explains what the imaging shows mechanically, whether decompression is a viable option, and what the overall treatment pathway looks like. This is a remote imaging review — not a physical examination. It costs you nothing and is available to Utah County residents.
Clinical Evidence
APFEL CC, ET AL., 2010
Non-surgical spinal decompression is associated with significant reduction in pain and disability in patients with lumbar disc herniation or degenerative disc disease.
RAMOS G, MARTIN W., 1994
Effects of vertebral axial decompression on intradiscal pressure demonstrated measurable reductions supporting therapeutic use.
GOSE EE, ET AL., 1998
Vertebral axial decompression therapy for pain associated with herniated or degenerated discs or facet syndrome showed significant clinical benefit.
References
- Apfel CC, et al. Non-surgical spinal decompression is associated with significant reduction in pain and disability in patients with lumbar disc herniation or degenerative disc disease. Pain Pract. 2010;10(3):167-78.
- Ramos G, Martin W. Effects of vertebral axial decompression on intradiscal pressure. J Neurosurg. 1994;81(3):350-3.
- Gose EE, et al. Vertebral axial decompression therapy for pain associated with herniated or degenerated discs or facet syndrome. Neurol Res. 1998;20(3):186-90.
Find Out If Decompression Is Right for You
Not every disc herniation needs surgery. Not every disc herniation needs decompression. What every disc herniation needs is an accurate mechanical evaluation that explains what is driving the problem and what the correct treatment sequence is. That is what we do.
Decompression works best as part of a complete plan. See the full Disc Recovery Program, which combines decompression with Class IV laser therapy and corrective care.
Serving Provo, Orem, Springville, Mapleton, Vineyard, Spanish Fork, and all of Utah County
Related Spine Conditions We Treat
Fellowship-trained care across Provo & Utah County. Explore related conditions:
More From Our Spine Education Library
Articles from our fellowship-trained doctors on the topics above:
Frequently Asked Questions
Does non-surgical spinal decompression work?
For the right candidate, yes. It eases pressure on the disc and nerve, which can reduce pain and improve function. We confirm the diagnosis with imaging so we treat the actual problem.
Is spinal decompression safe?
It is non-surgical and well tolerated for most people. Our doctors review your history and imaging first to make sure it is appropriate for you.
How many sessions will I need?
Most plans run over several weeks. The number depends on your disc, your symptoms, and how you respond, which we measure as we go.
Who is a candidate for spinal decompression?
People with disc herniation, sciatica, or disc-related back or neck pain are often good candidates. An MRI review tells us whether it fits your case.
Is decompression better than surgery?
For many disc problems, a non-surgical trial is a reasonable first step before considering surgery. Our doctors give you an honest read on all of your options, including referral when surgery is the better path.
Keep the results after decompression
Decompression relieves the disc. Stability retraining keeps it relieved. Our computerized spine stability program is the natural next phase: objective testing and force-feedback retraining so the pressure stays off your disc.